

Intra-articular Versus Extra-articular Coracoid Grafts: A Systematic Review of Capsular Repair Techniques During the Latarjet Procedure
- PMID: 35097145
- PMCID: PMC8793475
- DOI: 10.1177/23259671211068371
Intra-articular Versus Extra-articular Coracoid Grafts: A Systematic Review of Capsular Repair Techniques During the Latarjet Procedure
Abstract
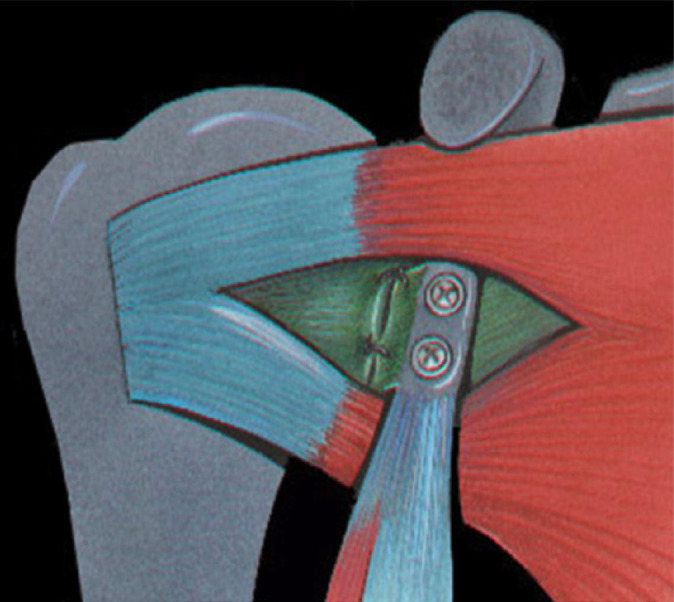
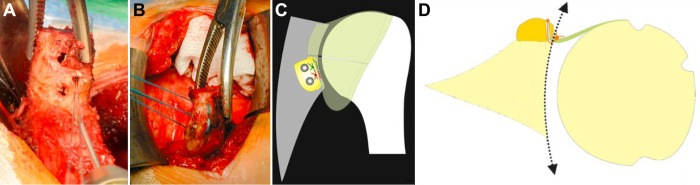
Background: Various methods exist for managing the joint capsule during the Latarjet procedure. Repairing the capsule to the native glenoid rim results in an extra-articular bone block, while repairing it to the remnant coracoacromial ligament stump of the coracoid graft renders it intra-articular. The technique that optimizes patient outcomes is not well defined.
Purpose: To compare the outcomes of intra-articular and extra-articular bone block techniques for the Latarjet procedure.
Study design: Systematic review; Level of evidence, 4.
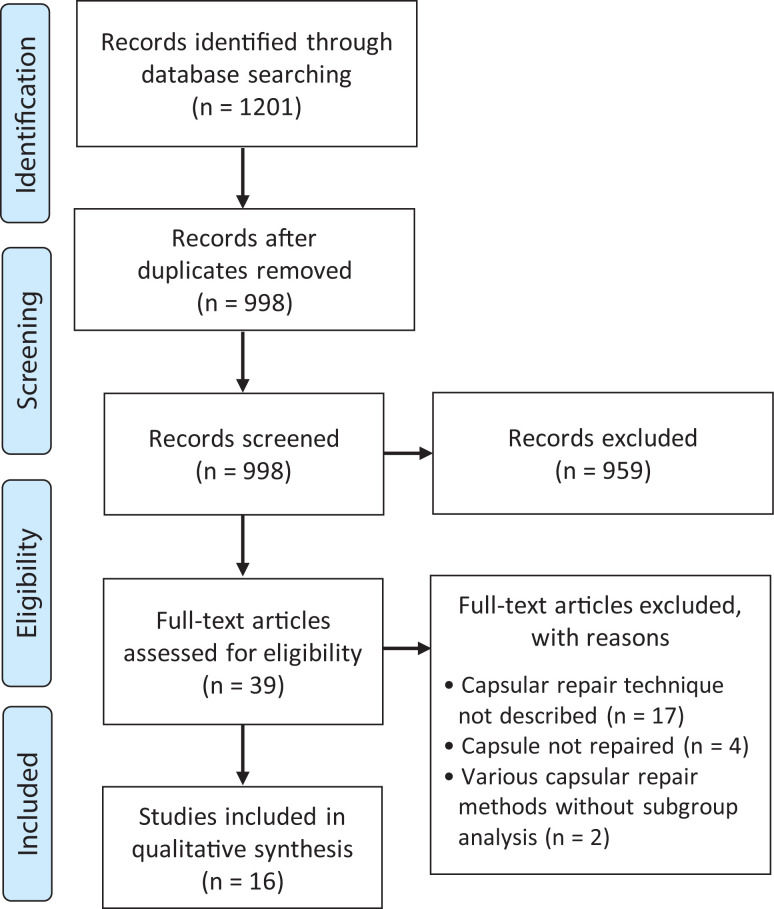
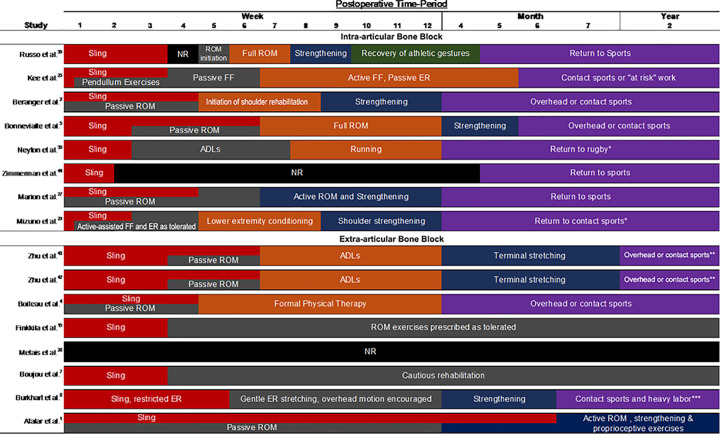
Methods: Using PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analyses) guidelines, we queried the PubMed, EMBASE, and the Cochrane Library for all studies reporting outcomes of the Latarjet procedure with a clearly defined method of capsular repair that rendered the coracoid graft intra-articular or extra-articular. The included levels of evidence and degree of heterogeneity in this study precluded meta-analysis. Outcomes of interest included preoperative variables, surgical technique, rehabilitation protocols, functional outcome assessments, recurrent instability, range of motion, and radiographic findings.
Results: A total of 16 studies including 816 patients were included. A total of 8 studies employed an intra-articular bone block in 338 patients, while the other 8 employed an extra-articular technique in 478 patients. There was variation among studies in reference to baseline patient characteristics, surgical techniques, rehabilitation, methods for assessing patient outcomes, and follow-up times. Rates of postoperative instability were reported in 8 intra-articular (0%, 0%, 2.1%, 2.7%, 3.2%, 5%, 5.4%, 5.9%) and 7 extra-articular (0%, 0%, 1.2%, 2%, 3.9%, 6.3%, 14%) bone block studies. Postoperative osteoarthritis or progression of preoperative osteoarthritis was reported in 5 intra-articular bone block studies (0%, 5.6%, 23.5%, 23.5%, 25%) and 4 extra-articular bone block studies (0%, 1.9%, 5.2%, 8.6%).
Conclusion: Varying capsular repair methods appeared to provide similar outcomes regarding stability. There was an apparent trend toward higher rates of post-traumatic arthritis among studies in which an intra-articular bone block technique was employed; however, it is possible that this was influenced by substantially different follow-up times between groups and other various sources of heterogeneity among the included studies. There were no studies in the literature directly comparing intra-articular and extra-articular bone block techniques. Large-scale randomized controlled trials or comparative studies are needed to draw stronger conclusions comparing the 2 techniques.
Keywords: Latarjet; glenoid reconstruction; osteoarthritis; shoulder instability.
© The Author(s) 2022.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: K.C.D. has received education payments from Gemini Mountain. M.T.P. has received research support from Arthrex, consulting fees from Arthrex and JRF (Allosource), nonconsulting fees from Arthrex and Flexion, and royalties from Arthrex and Arthrosurface. A.A.R. has received research support, consulting fees, nonconsulting fees, and royalties from Arthrex. K.B.F. has received education payments from Liberty Surgical, consulting fees from DePuy/Medical Device Business Services and Vericel, and nonconsulting fees from Aastrom Biosciences and Vericel. R.M.F. has received research support from Arthrex, education payments from Gemini Mountain and Smith & Nephew, consulting fees from Arthrex and JRF (Allosource), and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
Similar articles
-
Outcomes of the Latarjet Procedure Versus Free Bone Block Procedures for Anterior Shoulder Instability: A Systematic Review and Meta-analysis.Am J Sports Med. 2021 Mar;49(3):805-816. doi: 10.1177/0363546520925833. Epub 2020 Aug 14. Am J Sports Med. 2021. PMID: 32795174
-
Outcomes After Revision Anterior Shoulder Stabilization: A Systematic Review.Orthop J Sports Med. 2020 May 29;8(5):2325967120922571. doi: 10.1177/2325967120922571. eCollection 2020 May. Orthop J Sports Med. 2020. PMID: 32528993 Free PMC article. Review.
-
Comprehensive Modified Latarjet Technique: What the Masters Taught Us.JBJS Essent Surg Tech. 2021 Aug 27;11(3):e20.00049. doi: 10.2106/JBJS.ST.20.00049. eCollection 2021 Jul-Sep. JBJS Essent Surg Tech. 2021. PMID: 34650829 Free PMC article.
-
Arthroscopic Bankart repair with remplissage versus Latarjet procedure for management of engaging Hill-Sachs lesions with subcritical glenoid bone loss in traumatic anterior shoulder instability: a systematic review and meta-analysis.J Shoulder Elbow Surg. 2020 Oct;29(10):2163-2174. doi: 10.1016/j.jse.2020.04.032. Epub 2020 Jun 9. J Shoulder Elbow Surg. 2020. PMID: 32807370
-
Distal Clavicular Osteochondral Autograft Augmentation for Glenoid Bone Loss: A Comparison of Radius of Restoration Versus Latarjet Graft.Am J Sports Med. 2018 Apr;46(5):1046-1052. doi: 10.1177/0363546517749915. Epub 2018 Jan 30. Am J Sports Med. 2018. PMID: 29382209
Cited by
-
A comparative study of the effect of capsular repair in the Latarjet procedure.BMC Musculoskelet Disord. 2025 Jan 25;26(1):83. doi: 10.1186/s12891-025-08278-8. BMC Musculoskelet Disord. 2025. PMID: 39856648 Free PMC article.
-
Surgical Variations of the Modified Latarjet Procedure: A Literature Review and Video-Illustrated Surgical Technique.Cureus. 2024 Sep 25;16(9):e70221. doi: 10.7759/cureus.70221. eCollection 2024 Sep. Cureus. 2024. PMID: 39469396 Free PMC article. Review.
-
Latarjet procedure without capsular repair produces favorable clinical results and avoids limitation in external rotation.Knee Surg Sports Traumatol Arthrosc. 2023 Jul;31(7):2662-2669. doi: 10.1007/s00167-023-07393-0. Epub 2023 Mar 23. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 36951982
-
Global Research Trends in the Latarjet Procedure: A Bibliometric and Visualized Study.Medicina (Kaunas). 2022 Jul 28;58(8):1008. doi: 10.3390/medicina58081008. Medicina (Kaunas). 2022. PMID: 36013475 Free PMC article. Review.
References
-
- Atalar AC, Bilsel K, Eren I, Celik D, Cil H, Demirhan M. Modified Latarjet procedure for patients with glenoid bone defect accompanied with anterior shoulder instability. Acta Orthop Traumatol Turc. 2013;47(6):393–399. - PubMed
-
- Beranger JS, Klouche S, Bauer T, Demoures T, Hardy P. Anterior shoulder stabilization by Bristow-Latarjet procedure in athletes: return-to-sport and functional outcomes at minimum 2-year follow-up. Eur J Orthop Surg Traumatol. 2016;26(3):277–282. - PubMed
-
- Bigliani LU, Weinstein DM, Glasgow MT, Pollock RG, Flatow EL. Glenohumeral arthroplasty for arthritis after instability surgery. J Shoulder Elbow Surg. 1995;4(2):87–94. - PubMed
-
- Bonnevialle N, Ibnoulkhatib A, Mansat P, Rongieres M, Mansat M, Bonnevialle P. Outcomes of two surgical revision techniques for recurrent anterior shoulder instability following selective capsular repair. Orthop Traumatol Surg Res. 2013;99(4):455–463. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
