

Anatomy of the Distal End of Flexor Digitorum Longus Tendon and Percutaneous Release Technique: A Cadaveric Study
- PMID: 35097346
- PMCID: PMC8697276
- DOI: 10.1177/2473011419884274
Anatomy of the Distal End of Flexor Digitorum Longus Tendon and Percutaneous Release Technique: A Cadaveric Study
Abstract
Background: The transfer of flexor-to-extensor is widely used to correct lesser toe deformity and joint instability. The flexor digitorum longus tendon (FDLT) is percutaneously transected at the distal end and then routed dorsally to the proximal phalanx. The transected tendon must have enough mobility and length for the transfer. The purpose of this study was to dissect the distal end of FDLT and identify the optimal technique to percutaneously release FDLT.
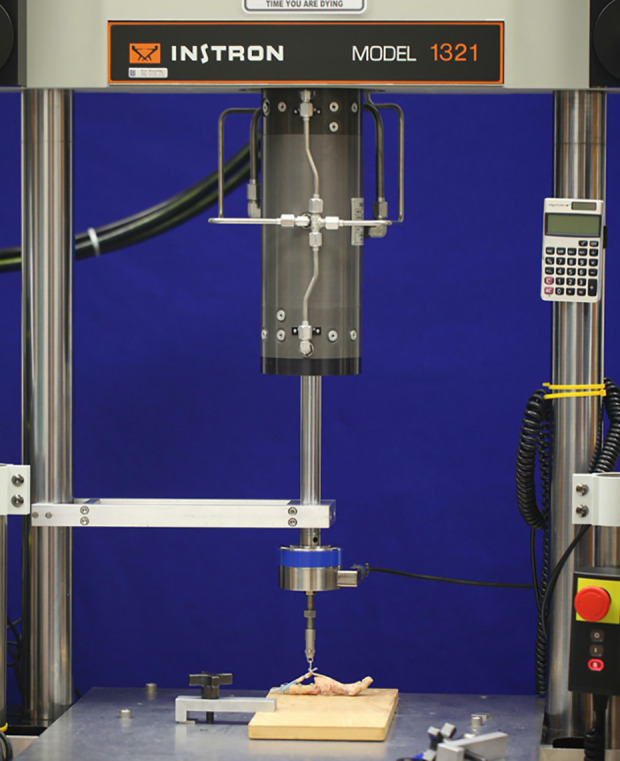
Methods: Eight fresh adult forefoot specimens were dissected to describe the relationship between the tendon and the neurovascular bundle and measure the width and length of the distal end of FDLT. Another 7 specimens were used to create the percutaneous release model and test the strength required to pull out FDLT proximally. The tendons were randomly released at the base of the distal phalanx (BDP), the space of the distal interphalangeal joint (SDIP), and the neck of the middle phalanx (NMP).
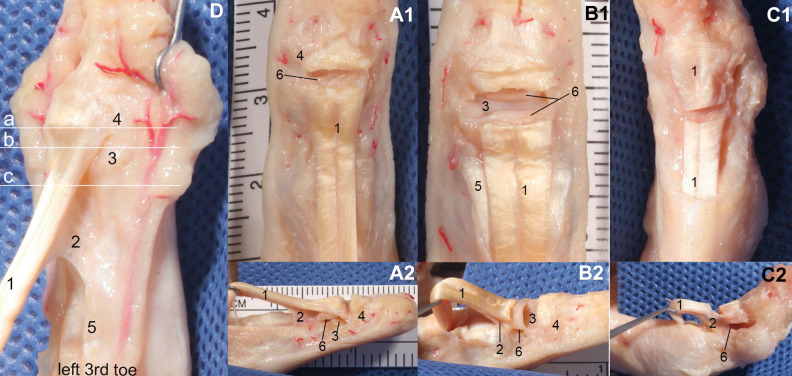
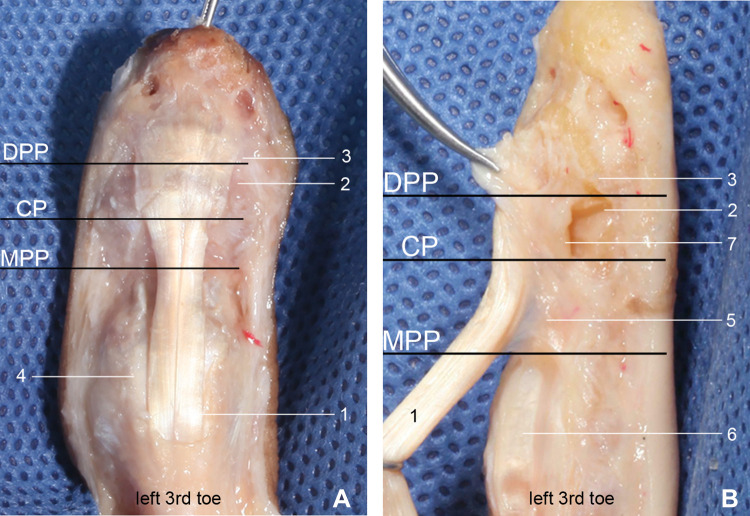
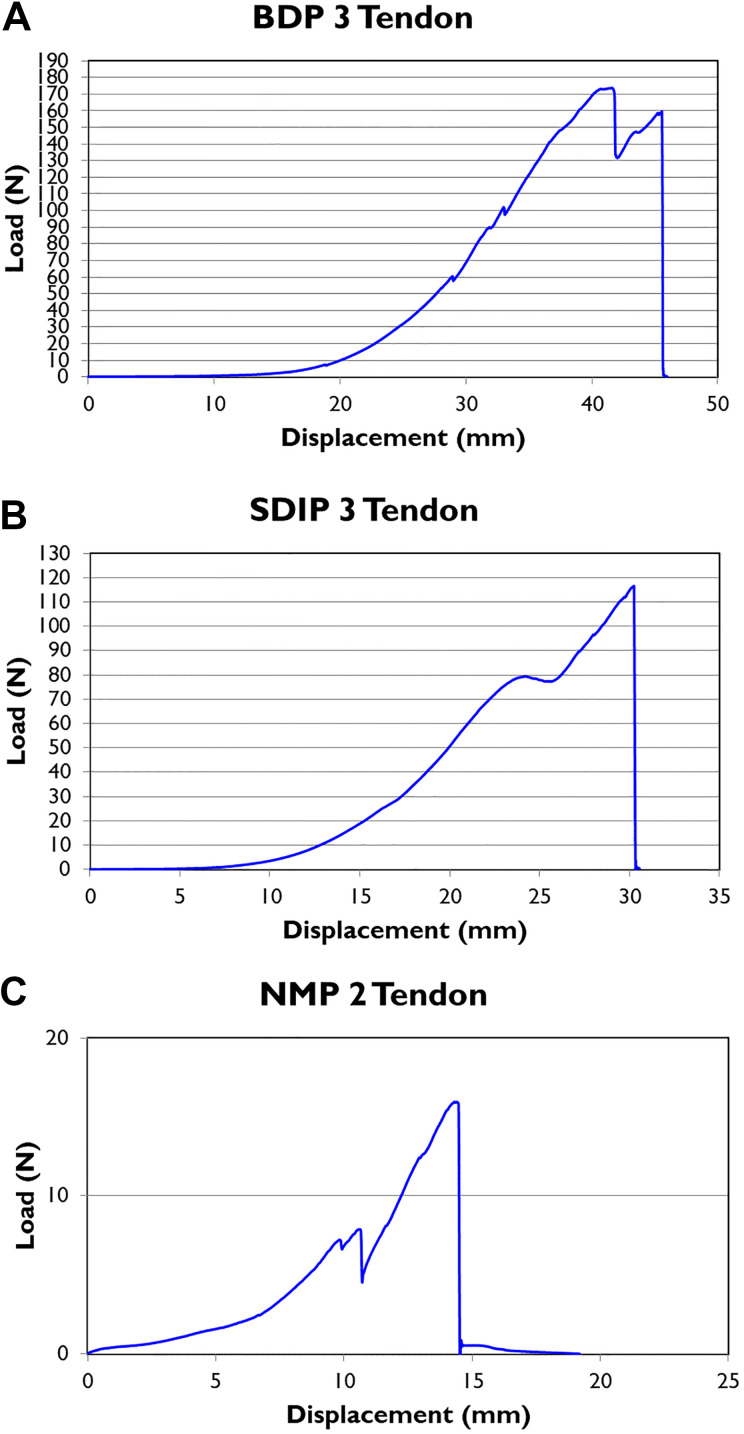
Results: At the distal interphalangeal (DIP) joint, the neurovascular bundle begins to migrate toward the center of the toe and branches off toward the center of the toe belly. The distal end of FDLT can be divided into 3 parts: the distal phalanx part (DPP), the capsule part (CP), and the middle phalanx part (MPP). There was a significant difference in width and length among the 3 parts. The strength required to pull out FDLT proximally was about 168, 96, and 20 N, respectively, for BDP, SDIP, and NMP.
Conclusion: The distal end of FDLT can be anatomically described at 3 locations: DPP, CP, and MPP. The tight vinculum brevis and the distal capsule are strong enough to resist proximal retraction. Percutaneous release at NMP can be performed safely and effectively.
Clinical relevance: Percutaneous release at NMP can be performed safely and effectively during flexor-to-extensor transfer.
Keywords: BDP; FDLT; NMP; plantar capsule; vinculum brevis.
© The Author(s) 2019.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Figures

Similar articles
-
Fifth-Toe Deformities.2022 Nov 19. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2022 Nov 19. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 32491393 Free Books & Documents.
-
Advantages and drawbacks of proximal interphalangeal joint fusion versus flexor tendon transfer in the correction of hammer and claw toe deformity. A finite-element study.J Biomech Eng. 2010 May;132(5):051002. doi: 10.1115/1.4001115. J Biomech Eng. 2010. PMID: 20459203
-
[Correction of flexible lesser toe deformity : Transfer of the flexor digitorum longus tendon].Oper Orthop Traumatol. 2017 Oct;29(5):452-458. doi: 10.1007/s00064-017-0511-y. Epub 2017 Jul 4. Oper Orthop Traumatol. 2017. PMID: 28676916 German.
-
[Minimally invasive correction of lesser toe deformities and treatment of metatarsalgia].Oper Orthop Traumatol. 2018 Jun;30(3):171-183. doi: 10.1007/s00064-018-0548-6. Epub 2018 May 8. Oper Orthop Traumatol. 2018. PMID: 29737368 Review. German.
-
The Accommodation of Bone Anchors Within the Distal Phalanx for Repair of Flexor Digitorum Profundus Avulsions.J Hand Surg Am. 2019 Nov;44(11):986.e1-986.e6. doi: 10.1016/j.jhsa.2018.12.012. Epub 2019 Feb 15. J Hand Surg Am. 2019. PMID: 30777399 Review.
References
-
- Arbab D, Frank D, Bouillon B, Lüring C. Behandlung flexibler leinzehenfeh- lstellungen: transfer der flexor-digitorum-longus-sehne [Correction of flexible lesser toe deformity : Transfer of the flexor digitorum longus tendon]. Oper Orthop Traumatol. 2017;29(5):452–458. - PubMed
-
- Bouché RT, Heit EJ. Combined plantar plate and hammertoe repair with flexor digitorum longus tendon transfer for chronic, severe sagittal plane instability of the lesser metatarsophalangeal joints: preliminary observations. J Foot Ankle Surg. 2008;47(2):125–137. - PubMed
-
- Boyer ML, DeOrio JK. Transfer of the flexor digitorum longus for the correction of lesser-toe deformities. Foot Ankle Int. 2016;28(4):422–430. - PubMed
-
- Butterworth M. Tendon transfers for management of digital and lesser metatarsophalangeal joint deformities. Clin Podiatr Med Surg. 2016;33(1):71–84. - PubMed
-
- Flindall E, Mcgrouther DA. Accessory roles of the vinculum breve of the flexor digitorum profundus and Check-Rein ligaments at the distal interphalangeal joint. J Hand Surg Br. 1991;16(3):305–310. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous