

Evaluation and Treatment of Chronic Plantar Fasciitis
- PMID: 35097359
- PMCID: PMC8564931
- DOI: 10.1177/2473011419896763
Evaluation and Treatment of Chronic Plantar Fasciitis
Abstract
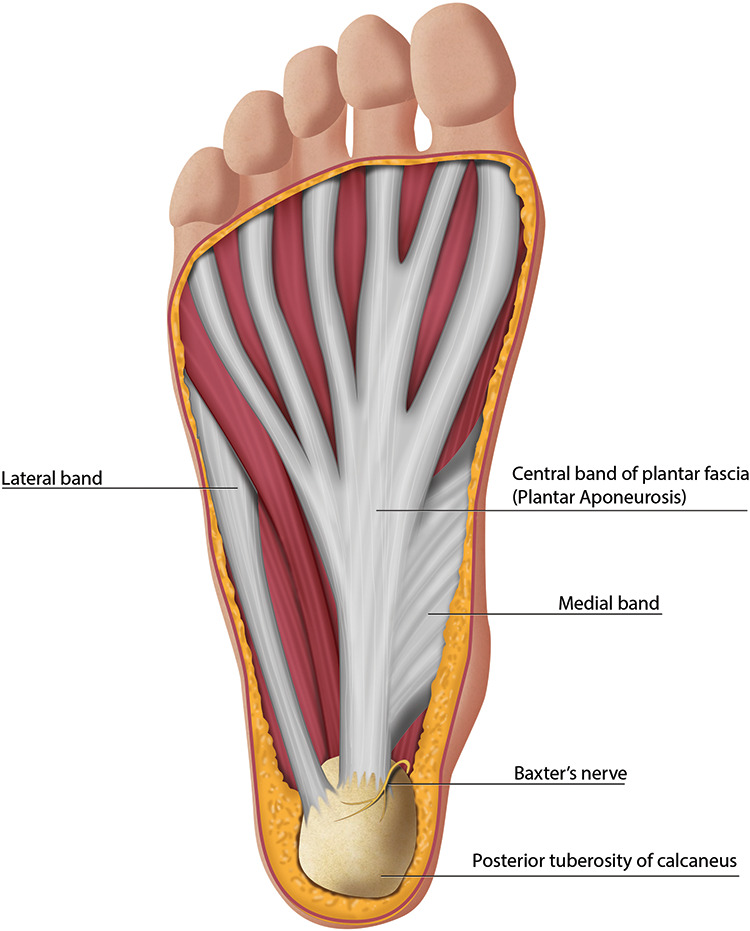
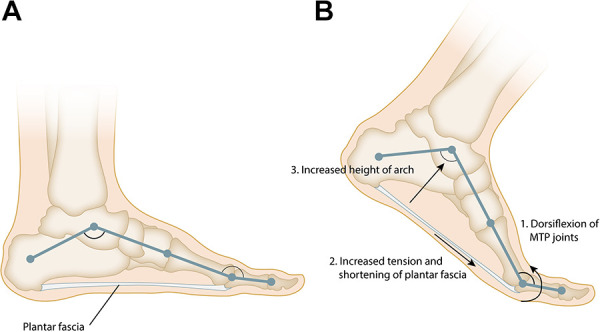
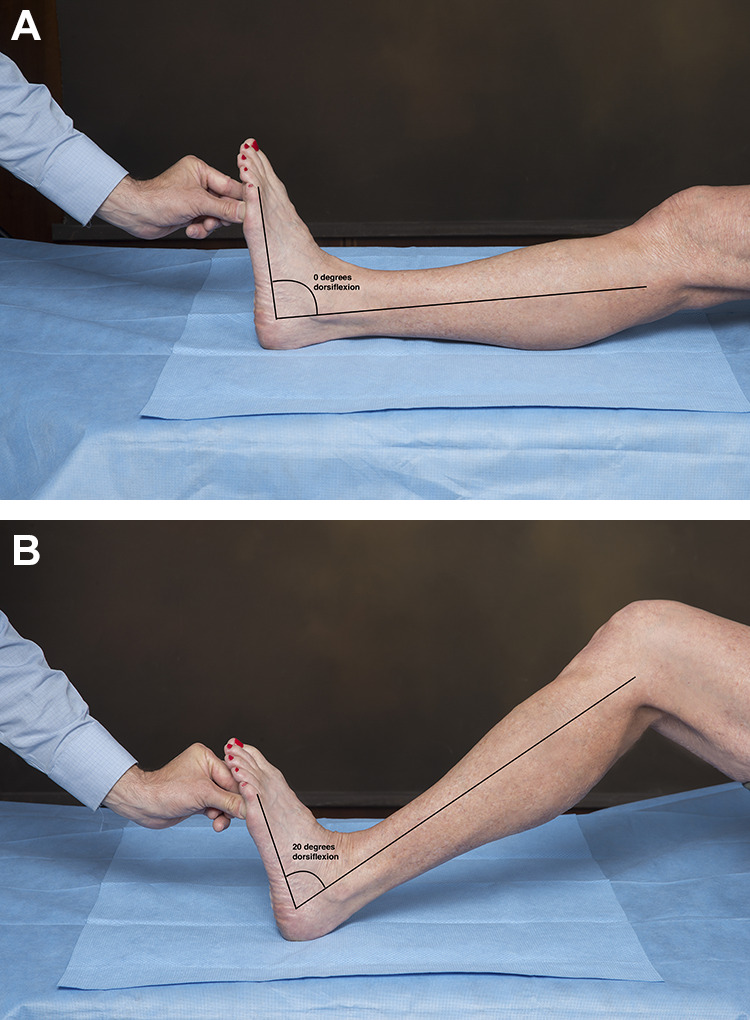
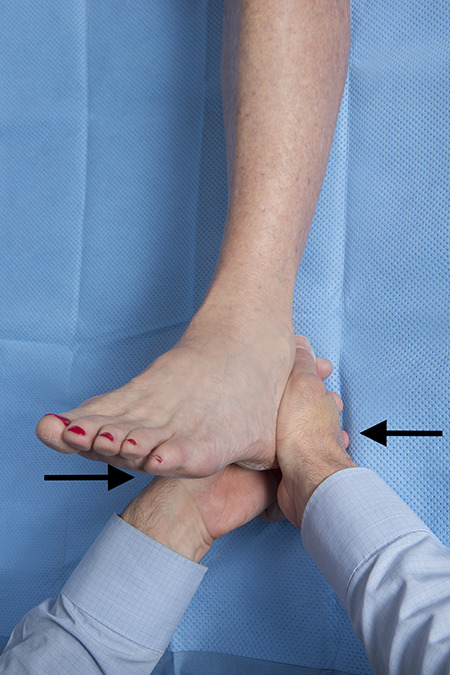
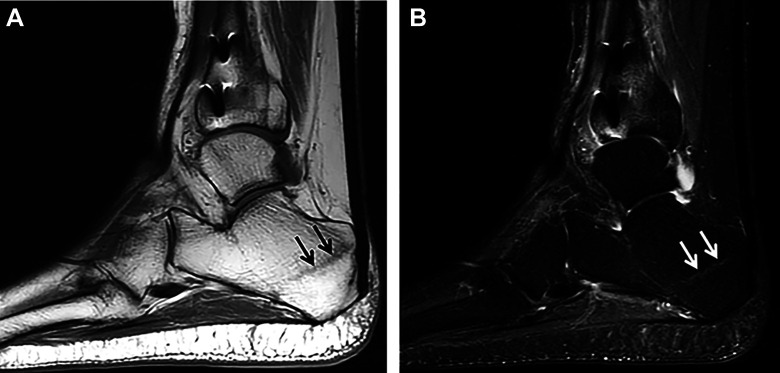
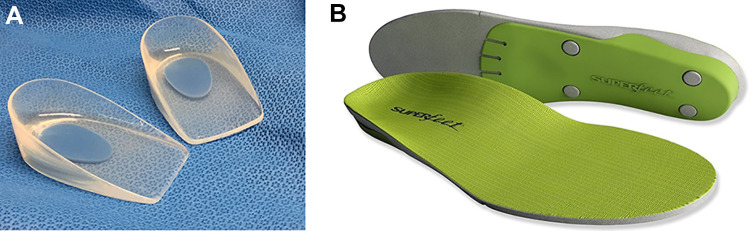
Plantar fasciitis is the most common cause of chronic heel pain in adults, affecting both young active patients and older sedentary individuals. It results from repetitive stress to the plantar fascia at its origin on the medial tubercle of the calcaneus and is often associated with gastrocnemius tightness. The diagnosis can be made clinically with a focused history and physical examination; imaging is reserved for atypical presentations and those that do not respond to initial treatment. The most common presenting symptom is aching plantar heel pain, which is worst with first step in the morning or after periods of rest. Diagnosis is confirmed with point tenderness at the origin of the plantar fascia on the medial tubercle of the calcaneus. Initial treatment consists of activity modification, anti-inflammatory medication, gastrocnemius and plantar fascia stretching, and an in-shoe orthosis that lifts and cushions the heel. These nonoperative treatments lead to complete resolution of pain in 90% of patients but can take 3-6 months. Patients who remain symptomatic despite a 6-month trial of nonoperative therapy may be considered for minimally invasive treatment or surgery. Platelet-rich plasma injections and therapeutic ultrasound are among a number of minimally invasive treatments that stimulate the body's healing response. Corticosteroid injections temporarily relieve pain, but may increase the risk of plantar fascia rupture and fat pad atrophy. Botulinum toxin injections relax the calf muscles, which decreases the stress in the plantar fascia. Operative treatments include gastrocnemius recession and medial head of gastrocnemius release, which decrease the stress on the plantar fascia and partial planter fasciotomy, which stimulates a healing response.
Level of evidence: Level V, expert opinion.
Keywords: fasciosis; plantar fascia; tendinosis; tendon disorders.
© The Author(s) 2020.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Figures



References
-
- Abbassian A, Kohls-Gatzoulis J, Solan MC. Proximal medial gastrocnemius release in the treatment of recalcitrant plantar fasciitis. Foot Ankle Int. 2012;33(1):14–19. - PubMed
-
- Ahmad J, Ahmad SH, Jones K. Treatment of plantar fasciitis with botulinum toxin: a randomized, controlled study. Foot Ankle Int. 2017;38(1):1–7. - PubMed
-
- Alshami AM, Babri AS, Souvlis T, Coppieters MW. Biomechanical evaluation of two clinical tests for plantar heel pain: the dorsiflexion-eversion test for tarsal tunnel syndrome and the windlass test for plantar fasciitis. Foot Ankle Int. 2007;28(4):499–505. - PubMed
-
- Barton JK, Rice PS, Howard CC, et al. Structural and functional assessment of intense therapeutic ultrasound effects on partial Achilles tendon transection. In: Advanced Biomedical and Clinical Diagnostic and Surgical Guidance Systems XVI 2018, San Francisco, United States, January 28-30, 2018. Bellingham, WA: SPIE; 2018.
-
- Bazaz R, Ferkel RD. Results of endoscopic plantar fascia release. Foot Ankle Int. 2007;28(5):549–556. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical