

Prevalence Estimates of Amyloid Abnormality Across the Alzheimer Disease Clinical Spectrum
- PMID: 35099509
- PMCID: PMC12138908
- DOI: 10.1001/jamaneurol.2021.5216
Prevalence Estimates of Amyloid Abnormality Across the Alzheimer Disease Clinical Spectrum
Erratum in
-
Errors in the Author Affiliations and Figure 1 Legend.JAMA Neurol. 2022 Mar 1;79(3):313. doi: 10.1001/jamaneurol.2022.0265. JAMA Neurol. 2022. PMID: 35285880 Free PMC article. No abstract available.
Abstract
Importance: One characteristic histopathological event in Alzheimer disease (AD) is cerebral amyloid aggregation, which can be detected by biomarkers in cerebrospinal fluid (CSF) and on positron emission tomography (PET) scans. Prevalence estimates of amyloid pathology are important for health care planning and clinical trial design.
Objective: To estimate the prevalence of amyloid abnormality in persons with normal cognition, subjective cognitive decline, mild cognitive impairment, or clinical AD dementia and to examine the potential implications of cutoff methods, biomarker modality (CSF or PET), age, sex, APOE genotype, educational level, geographical region, and dementia severity for these estimates.
Design, setting, and participants: This cross-sectional, individual-participant pooled study included participants from 85 Amyloid Biomarker Study cohorts. Data collection was performed from January 1, 2013, to December 31, 2020. Participants had normal cognition, subjective cognitive decline, mild cognitive impairment, or clinical AD dementia. Normal cognition and subjective cognitive decline were defined by normal scores on cognitive tests, with the presence of cognitive complaints defining subjective cognitive decline. Mild cognitive impairment and clinical AD dementia were diagnosed according to published criteria.
Exposures: Alzheimer disease biomarkers detected on PET or in CSF.
Main outcomes and measures: Amyloid measurements were dichotomized as normal or abnormal using cohort-provided cutoffs for CSF or PET or by visual reading for PET. Adjusted data-driven cutoffs for abnormal amyloid were calculated using gaussian mixture modeling. Prevalence of amyloid abnormality was estimated according to age, sex, cognitive status, biomarker modality, APOE carrier status, educational level, geographical location, and dementia severity using generalized estimating equations.
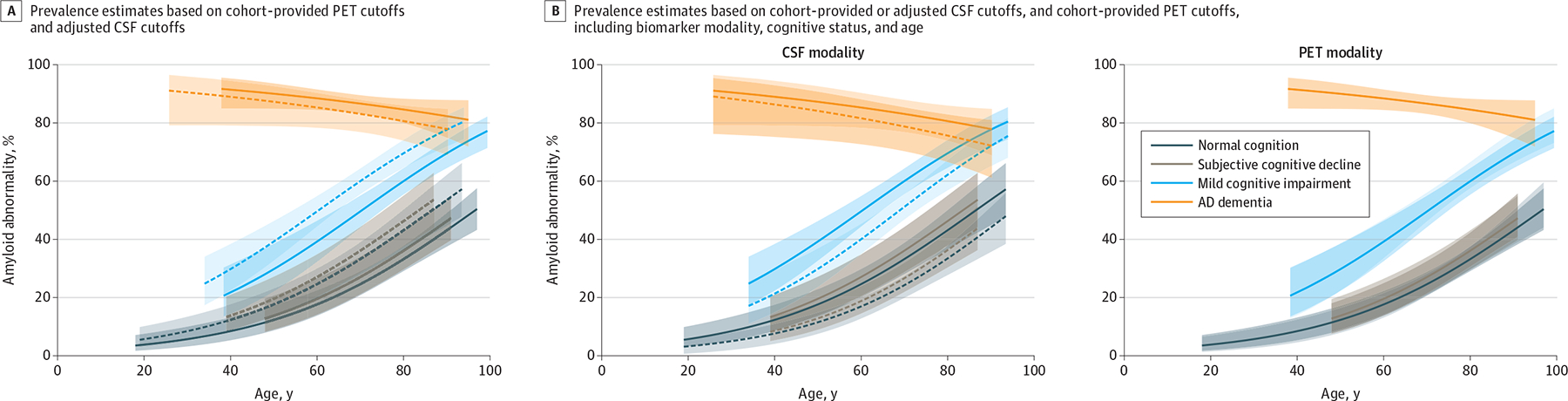
Results: Among the 19 097 participants (mean [SD] age, 69.1 [9.8] years; 10 148 women [53.1%]) included, 10 139 (53.1%) underwent an amyloid PET scan and 8958 (46.9%) had an amyloid CSF measurement. Using cohort-provided cutoffs, amyloid abnormality prevalences were similar to 2015 estimates for individuals without dementia and were similar across PET- and CSF-based estimates (24%; 95% CI, 21%-28%) in participants with normal cognition, 27% (95% CI, 21%-33%) in participants with subjective cognitive decline, and 51% (95% CI, 46%-56%) in participants with mild cognitive impairment, whereas for clinical AD dementia the estimates were higher for PET than CSF (87% vs 79%; mean difference, 8%; 95% CI, 0%-16%; P = .04). Gaussian mixture modeling-based cutoffs for amyloid measures on PET scans were similar to cohort-provided cutoffs and were not adjusted. Adjusted CSF cutoffs resulted in a 10% higher amyloid abnormality prevalence than PET-based estimates in persons with normal cognition (mean difference, 9%; 95% CI, 3%-15%; P = .004), subjective cognitive decline (9%; 95% CI, 3%-15%; P = .005), and mild cognitive impairment (10%; 95% CI, 3%-17%; P = .004), whereas the estimates were comparable in persons with clinical AD dementia (mean difference, 4%; 95% CI, -2% to 9%; P = .18).
Conclusions and relevance: This study found that CSF-based estimates using adjusted data-driven cutoffs were up to 10% higher than PET-based estimates in people without dementia, whereas the results were similar among people with dementia. This finding suggests that preclinical and prodromal AD may be more prevalent than previously estimated, which has important implications for clinical trial recruitment strategies and health care planning policies.
Figures

Comment in
-
Prevalence Rates of Amyloid Positivity-Updates and Relevance.JAMA Neurol. 2022 Mar 1;79(3):225-227. doi: 10.1001/jamaneurol.2021.5225. JAMA Neurol. 2022. PMID: 35099511 No abstract available.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
