

Deep learning-based artificial intelligence for prostate cancer detection at biparametric MRI
- PMID: 35099572
- PMCID: PMC10506420
- DOI: 10.1007/s00261-022-03419-2
Deep learning-based artificial intelligence for prostate cancer detection at biparametric MRI
Abstract
Purpose: To present fully automated DL-based prostate cancer detection system for prostate MRI.
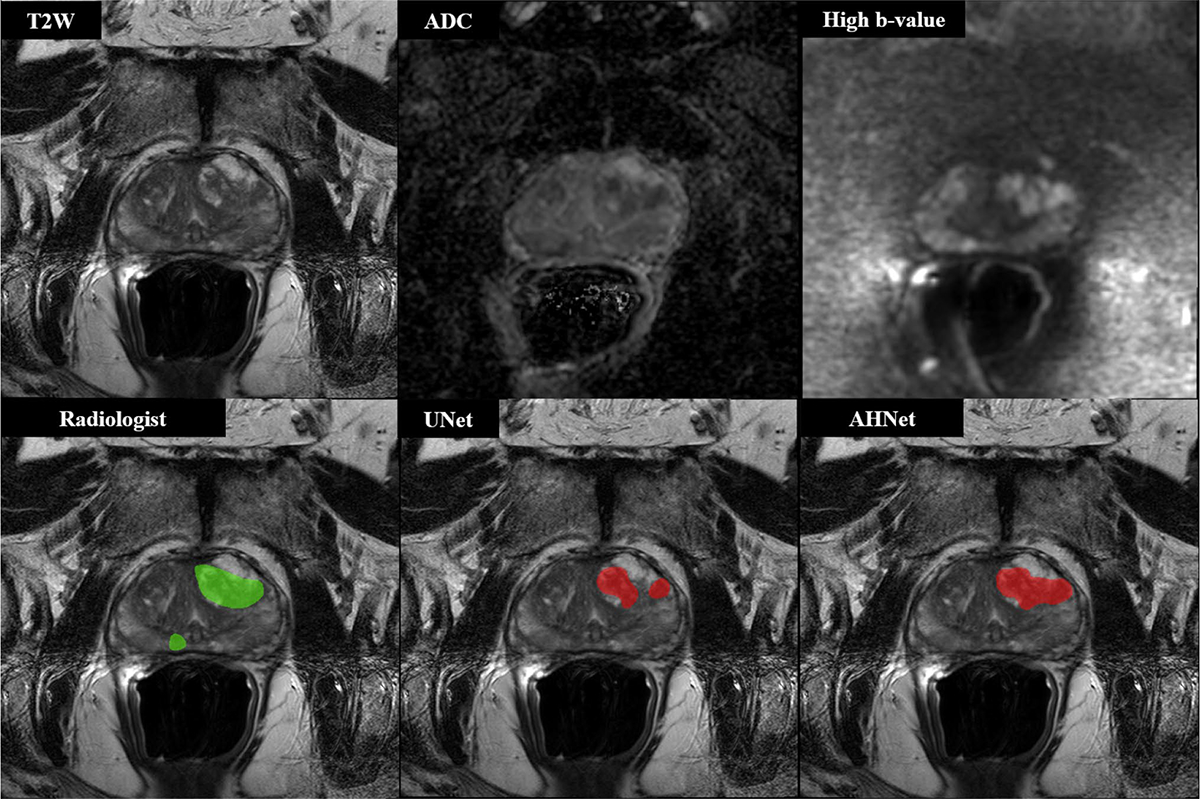
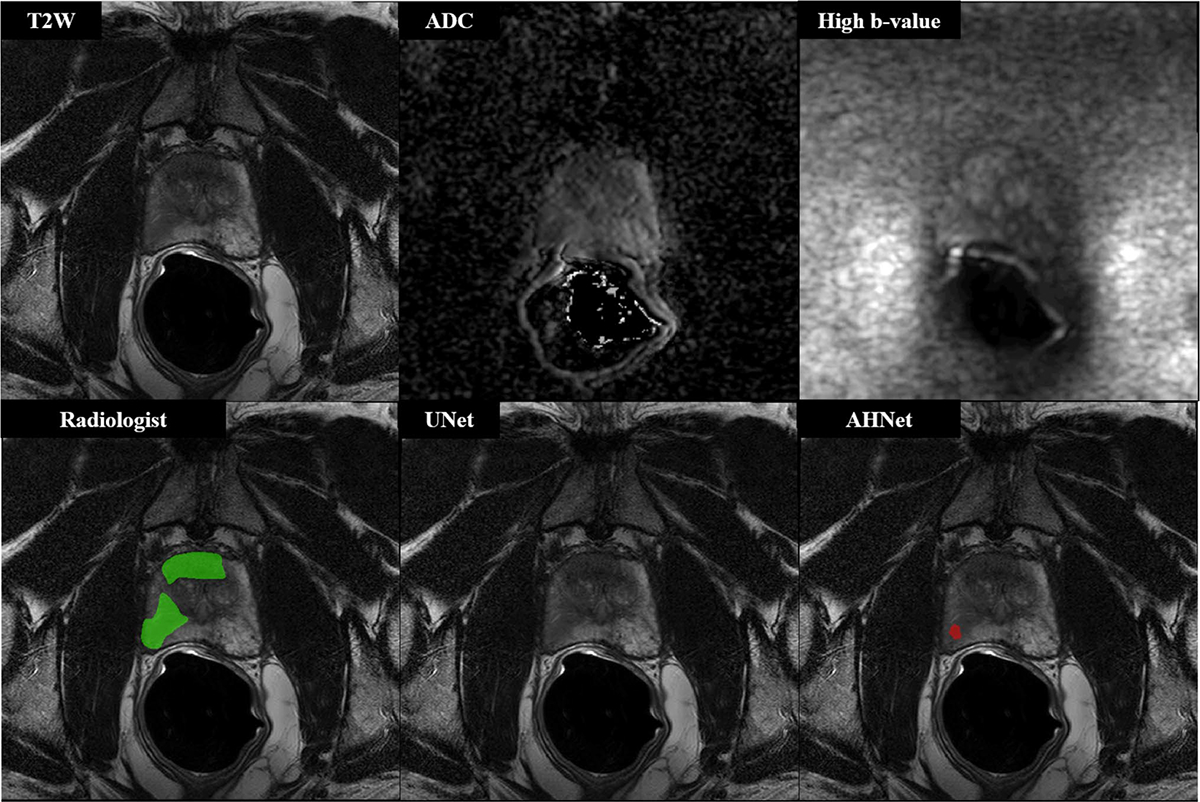
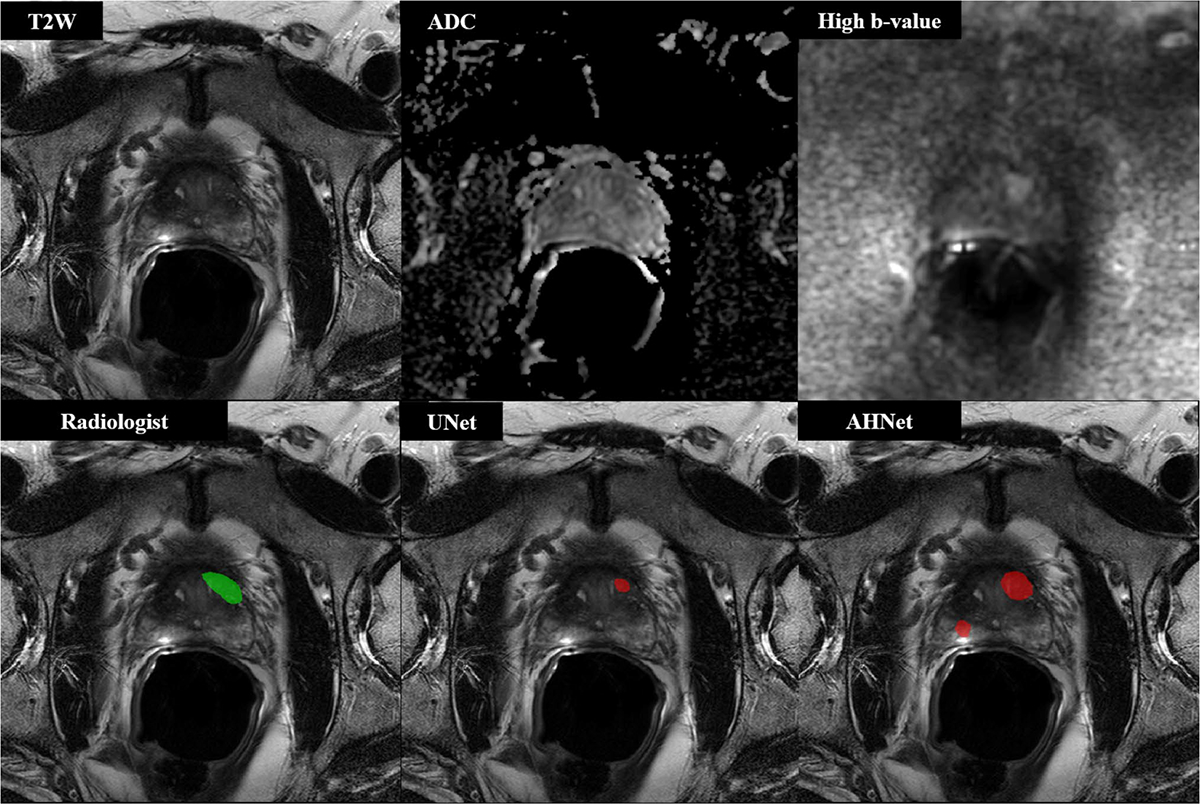
Methods: MRI scans from two institutions, were used for algorithm training, validation, testing. MRI-visible lesions were contoured by an experienced radiologist. All lesions were biopsied using MRI-TRUS-guidance. Lesions masks, histopathological results were used as ground truth labels to train UNet, AH-Net architectures for prostate cancer lesion detection, segmentation. Algorithm was trained to detect any prostate cancer ≥ ISUP1. Detection sensitivity, positive predictive values, mean number of false positive lesions per patient were used as performance metrics.
Results: 525 patients were included for training, validation, testing of the algorithm. Dataset was split into training (n = 368, 70%), validation (n = 79, 15%), test (n = 78, 15%) cohorts. Dice coefficients in training, validation sets were 0.403, 0.307, respectively, for AHNet model compared to 0.372, 0.287, respectively, for UNet model. In validation set, detection sensitivity was 70.9%, PPV was 35.5%, mean number of false positive lesions/patient was 1.41 (range 0-6) for UNet model compared to 74.4% detection sensitivity, 47.8% PPV, mean number of false positive lesions/patient was 0.87 (range 0-5) for AHNet model. In test set, detection sensitivity for UNet was 72.8% compared to 63.0% for AHNet, mean number of false positive lesions/patient was 1.90 (range 0-7), 1.40 (range 0-6) in UNet, AHNet models, respectively.
Conclusion: We developed a DL-based AI approach which predicts prostate cancer lesions at biparametric MRI with reasonable performance metrics. While false positive lesion calls remain as a challenge of AI-assisted detection algorithms, this system can be utilized as an adjunct tool by radiologists.
Keywords: Artificial intelligence; Deep learning; Magnetic resonance imaging; Prostate cancer.
© 2022. This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
