

Myocardial CT perfusion imaging for the detection of obstructive coronary artery disease: multisegment reconstruction does not improve diagnostic performance
- PMID: 35099638
- PMCID: PMC8804122
- DOI: 10.1186/s41747-021-00256-8
Myocardial CT perfusion imaging for the detection of obstructive coronary artery disease: multisegment reconstruction does not improve diagnostic performance
Abstract
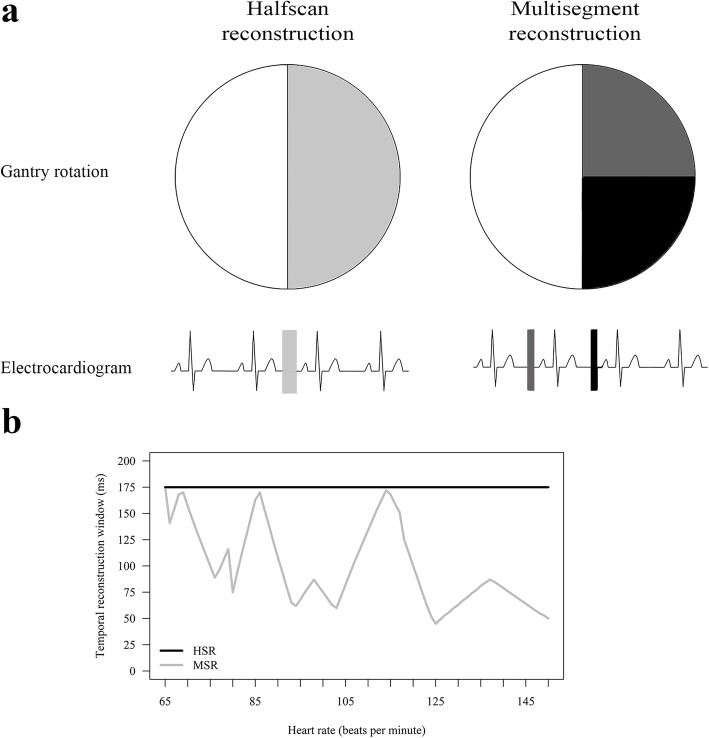
Background: Multisegment reconstruction (MSR) was introduced to shorten the temporal reconstruction window of computed tomography (CT) and thereby reduce motion artefacts. We investigated whether MSR of myocardial CT perfusion (CTP) can improve diagnostic performance in detecting obstructive coronary artery disease (CAD) compared with halfscan reconstruction (HSR).
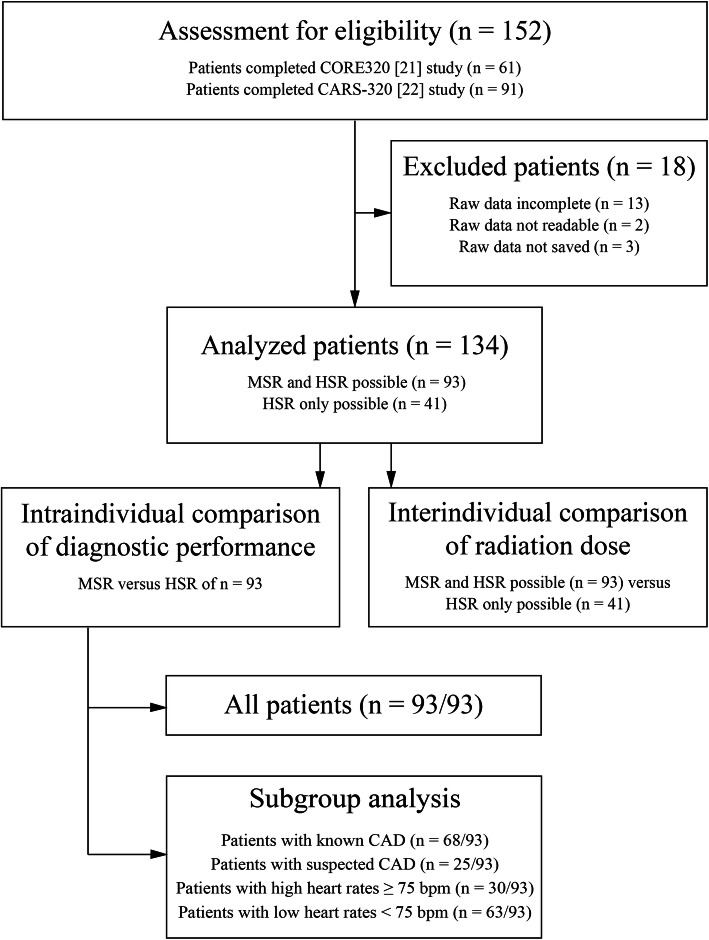
Methods: A total of 134 patients (median age 65.7 years) with clinical indication for invasive coronary angiography and without cardiac surgery prospectively underwent static CTP. In 93 patients with multisegment acquisition, we retrospectively performed both MSR and HSR and searched both reconstructions for perfusion defects. Subgroups with known (n = 68) or suspected CAD (n = 25) and high heart rate (n = 30) were analysed. The area under the curve (AUC) was compared applying DeLong approach using ≥ 50% stenosis on invasive coronary angiography as reference standard.
Results: Per-patient analysis revealed the overall AUC of MSR (0.65 [95% confidence interval 0.53, 0.78]) to be inferior to that of HSR (0.79 [0.69, 0.88]; p = 0.011). AUCs of MSR and HSR were similar in all subgroups analysed (known CAD 0.62 [0.45, 0.79] versus 0.72 [0.57, 0.86]; p = 0.157; suspected CAD 0.80 [0.63, 0.97] versus 0.89 [0.77, 1.00]; p = 0.243; high heart rate 0.46 [0.19, 0.73] versus 0.55 [0.33, 0.77]; p = 0.389). Median stress radiation dose was higher for MSR than for HSR (6.67 mSv versus 3.64 mSv, p < 0.001).
Conclusions: MSR did not improve diagnostic performance of myocardial CTP imaging while increasing radiation dose compared with HSR.
Trial registration: CORE320: clinicaltrials.gov NCT00934037, CARS-320: NCT00967876.
Keywords: Coronary angiography; Coronary artery disease; Multidetector computed tomography; Myocardial perfusion imaging; Sensitivity and specificity.
© 2022. The Author(s) under exclusive licence to European Society of Radiology.
Conflict of interest statement
Institutional master research agreements exist with Siemens, General Electric, Philips, and Canon Medical Systems (former Toshiba Medical Systems). The terms of these arrangements are managed by the legal department of Charité – Universitätsmedizin Berlin.
Prof. Dewey has received grant support from the FP7 Program of the European Commission for the randomized multicenter DISCHARGE trial (603266-2, HEALTH-2012.2.4.-2). He also received grant support from German Research Foundation (DFG) in the Heisenberg Program (DE 1361/14-1), graduate programme on quantitative biomedical imaging (BIOQIC, GRK 2260/1), for fractal analysis of myocardial perfusion (DE 1361/18-1), the Priority Programme Radiomics for the investigation of coronary plaque and coronary flow (DE 1361/19-1 [428222922] and 20-1 [428223139] in SPP 2177/1). He also received funding from the Berlin University Alliance (GC_SC_PC 27) and from the Digital Health Accelerator of the Berlin Institute of Health. Prof. Dewey has received lecture fees from Canon Medical Systems (former Toshiba Medical Systems), Guerbet. Prof. Dewey is European Society of Radiology (ESR) Research Chair (2019–2022) and the opinions expressed in this article are the author’s own and do not represent the view of ESR. Per the guiding principles of ESR, the work as Research Chair is on a voluntary basis and only travel expenses are remunerated. Prof. Dewey is also the editor of Cardiac CT, published by Springer Nature, and offers hands-on courses on CT imaging (
Dr. Rief received grant support for the investigation of coronary plaque from the ‘Radiomics’ Priority Programme of the German Research Foundation (DFG).
Other authors declared no conflicts of interest.
Figures


References
-
- Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2012;60:e44–e164. doi: 10.1016/j.jacc.2012.07.013. - DOI - PubMed
-
- Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34:2949–3003. doi: 10.1093/eurheartj/eht310.P4876. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous