

Transfusion-Associated Delirium in Children: No Difference Between Short Storage Versus Standard Issue RBCs
- PMID: 35100190
- PMCID: PMC8820396
- DOI: 10.1097/CCM.0000000000005393
Transfusion-Associated Delirium in Children: No Difference Between Short Storage Versus Standard Issue RBCs
Abstract
Objectives: Primary objective is to determine if transfusion of short storage RBCs compared with standard issue RBCs reduced risk of delirium/coma in critically ill children. Secondary objective is to assess if RBC transfusion was independently associated with delirium/coma.
Design: This study was performed in two stages. First, we compared patients receiving either short storage or standard RBCs in a multi-institutional prospective randomized controlled trial. Then, we compared all transfused patients in the randomized controlled trial with a single-center cohort of nontransfused patients matched for confounders of delirium/coma.
Setting: Twenty academic PICUs who participated in the Age of Transfused Blood in Critically Ill Children trial.
Patients: Children 3 days to 16 years old who were transfused RBCs within the first 7 days of admission.
Interventions: Subjects were randomized to either short storage RBC study arm (defined as RBCs stored for up to seven days) or standard issue RBC study arm. In addition, subjects were screened for delirium prior to transfusion and every 12 hours after transfusion for up to 3 days.
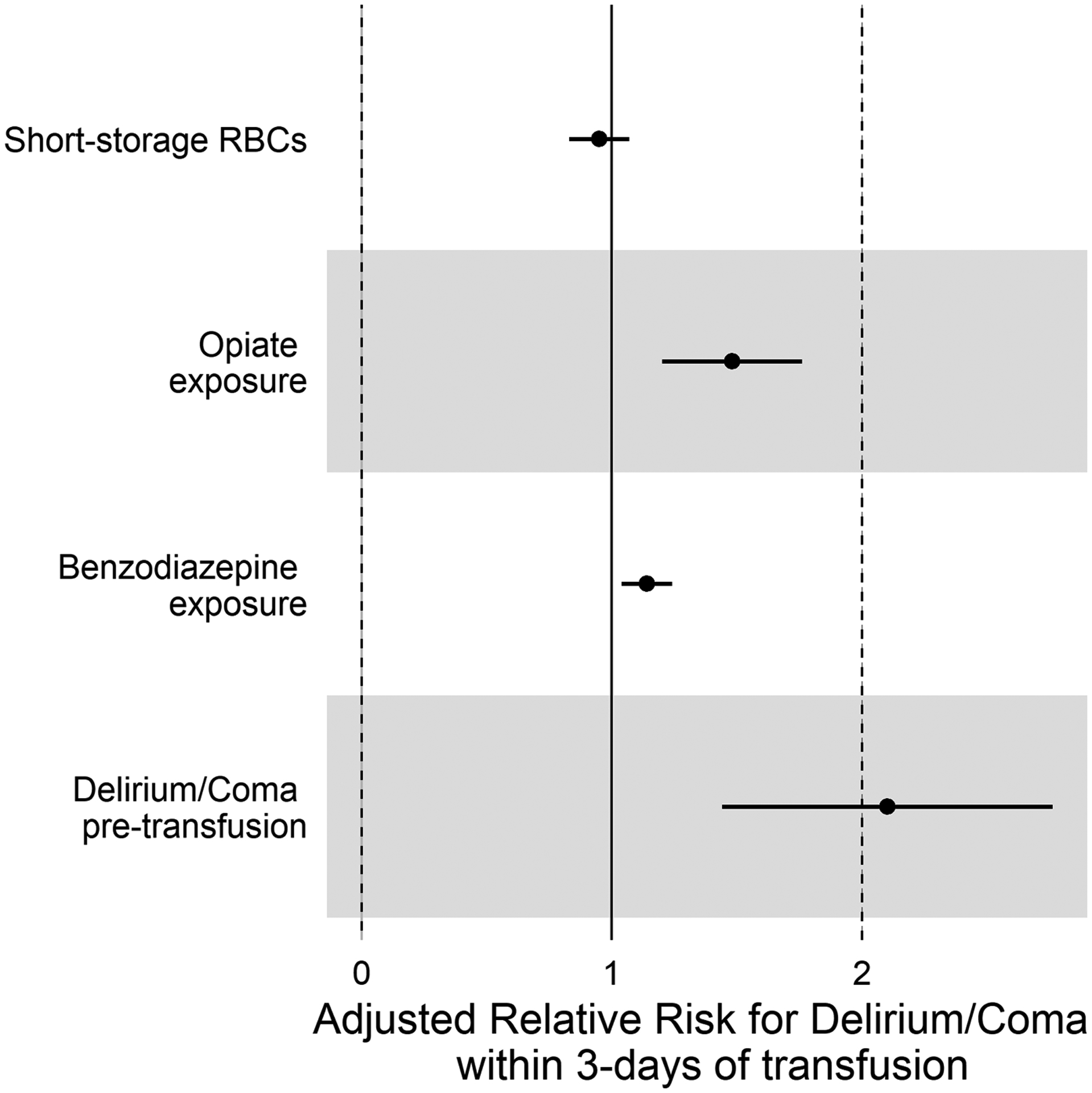
Measurements and main results: Primary outcome measure was development of delirium/coma within 3 days of initial transfusion. Additional outcome measures were dose-response relationship between volume of RBCs transfused and delirium/coma, and comparison of delirium/coma rates between transfused patients and individually matched nontransfused patients. We included 146 subjects in the stage I analysis; 69 were randomized to short storage RBCs and 77 to standard issue. There was no significant difference in delirium/coma development between study arms (79.5% vs 70.1%; p = 0.184). In the stage II analysis, adjusted odds for delirium in the transfused cohort was more than eight-fold higher than in the nontransfused matched cohort, even after controlling for hemoglobin (adjusted odds ratio, 8.9; CI, 2.8-28.4; p < 0.001).
Conclusions: RBC transfusions (and not anemia) are independently associated with increased odds of subsequent delirium/coma. However, storage age of RBCs does not affect delirium risk.
Copyright © 2022 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
Drs. Traube, Nellis, Avery, McQuillen, Fitzgerald, and Spinella received support for article research from the National Institutes of Health (NIH). Dr. Nellis’ institution received funding from the National Heart, Lung, and Blood Institute. Dr. McQuillen’s institution received funding from the National Institute of Child Health and Human Development. Dr. Fitzgerald’s institution received funding from the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Muszynski’s institution received funding from Washington University at St. Louis. Dr. Hanson’s institution received funding from the NIH. Dr. Lacroix’s institution received funding from the Canadian Institutes of Health Research. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. Arlington, VA, American Psychiatric Association, 2013. n.d.
