

Lung- and Diaphragm-Protective Ventilation by Titrating Inspiratory Support to Diaphragm Effort: A Randomized Clinical Trial
- PMID: 35100192
- PMCID: PMC8797006
- DOI: 10.1097/CCM.0000000000005395
Lung- and Diaphragm-Protective Ventilation by Titrating Inspiratory Support to Diaphragm Effort: A Randomized Clinical Trial
Abstract
Objectives: Lung- and diaphragm-protective ventilation is a novel concept that aims to limit the detrimental effects of mechanical ventilation on the diaphragm while remaining within limits of lung-protective ventilation. The premise is that low breathing effort under mechanical ventilation causes diaphragm atrophy, whereas excessive breathing effort induces diaphragm and lung injury. In a proof-of-concept study, we aimed to assess whether titration of inspiratory support based on diaphragm effort increases the time that patients have effort in a predefined "diaphragm-protective" range, without compromising lung-protective ventilation.
Design: Randomized clinical trial.
Setting: Mixed medical-surgical ICU in a tertiary academic hospital in the Netherlands.
Patients: Patients (n = 40) with respiratory failure ventilated in a partially-supported mode.
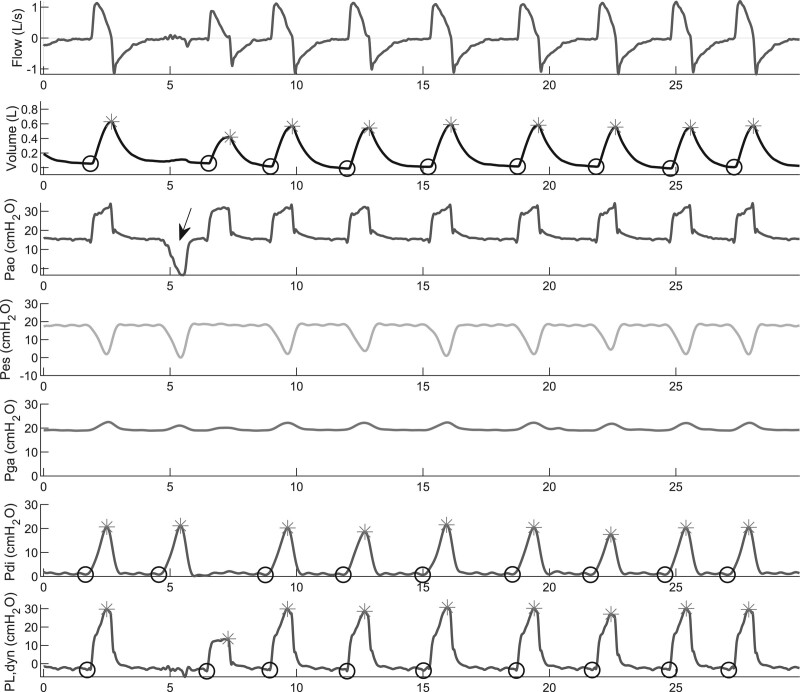
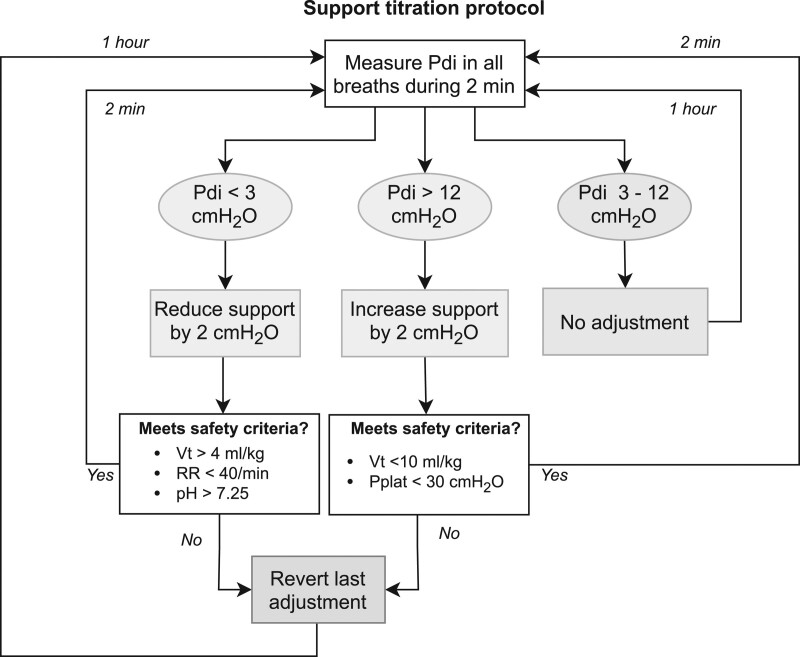
Interventions: In the intervention group, inspiratory support was titrated hourly to obtain transdiaphragmatic pressure swings in the predefined "diaphragm-protective" range (3-12 cm H2O). The control group received standard-of-care.
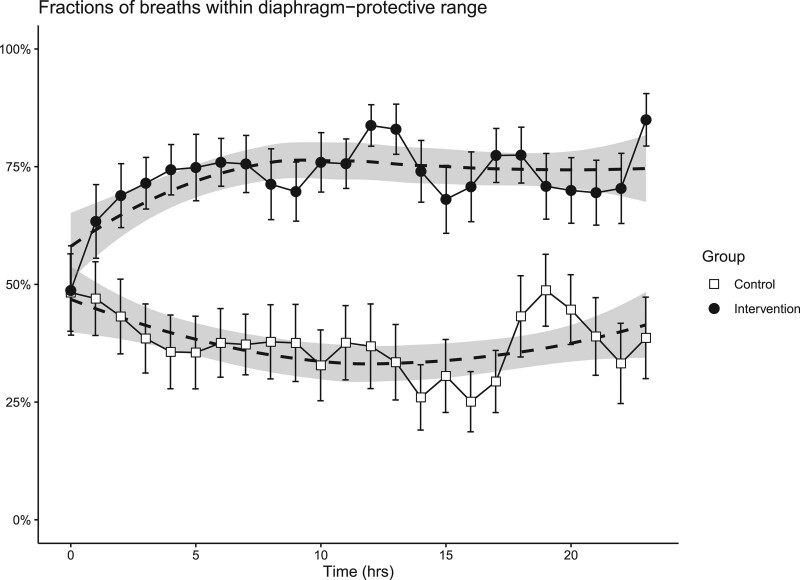
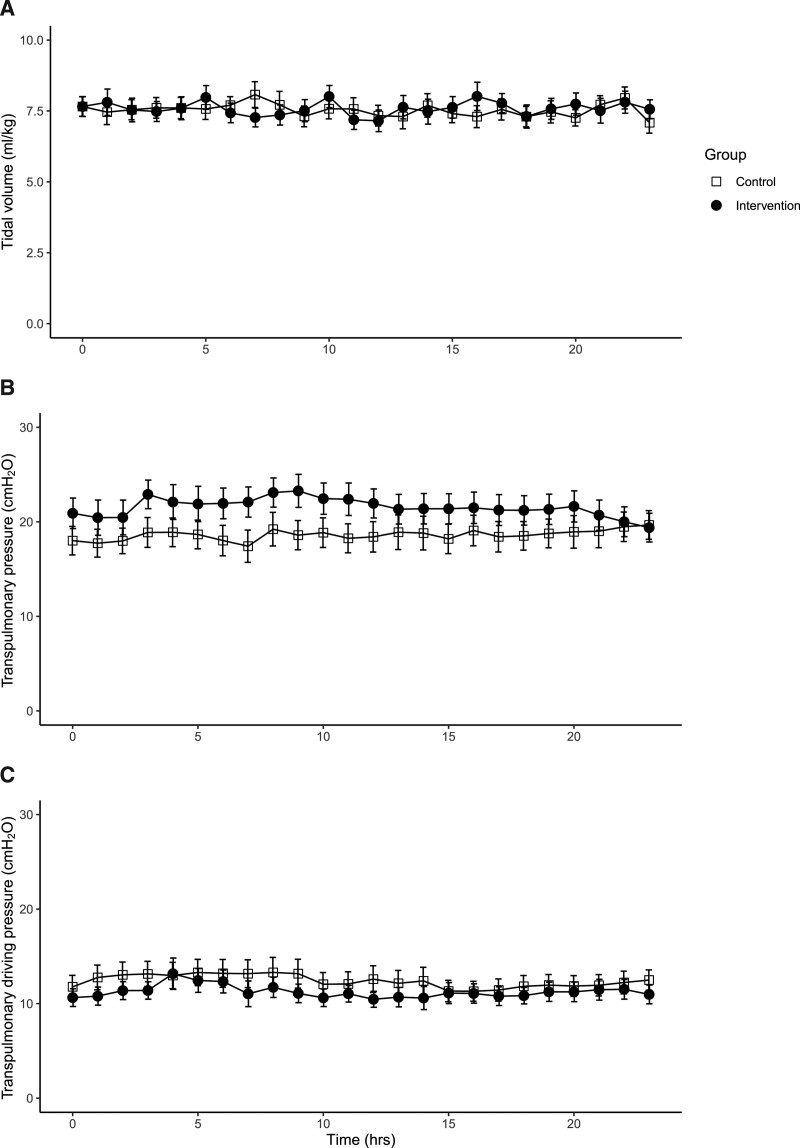
Measurements and main results: Transdiaphragmatic pressure, transpulmonary pressure, and tidal volume were monitored continuously for 24 hours in both groups. In the intervention group, more breaths were within "diaphragm-protective" range compared with the control group (median 81%; interquartile range [64-86%] vs 35% [16-60%], respectively; p < 0.001). Dynamic transpulmonary pressures (20.5 ± 7.1 vs 18.5 ± 7.0 cm H2O; p = 0.321) and tidal volumes (7.56 ± 1.47 vs 7.54 ± 1.22 mL/kg; p = 0.961) were not different in the intervention and control group, respectively.
Conclusions: Titration of inspiratory support based on patient breathing effort greatly increased the time that patients had diaphragm effort in the predefined "diaphragm-protective" range without compromising tidal volumes and transpulmonary pressures. This study provides a strong rationale for further studies powered on patient-centered outcomes.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and Wolters Kluwer Health, Inc.
Conflict of interest statement
Drs. de Vries’ and Heunks’ institutions received funding from Amsterdam Cardiovascular Sciences. Dr. de Vries has received speaker fees from the Dutch Ultrasound Center (the Netherlands) and travel and speaker fees from the Chinese Organization of Rehabilitation Medicine (China). Dr. Jonkman has received personal fees from Liberate Medical (United States). Dr. Heunks received research support from Liberate Medical (United States), Fisher and Paykel, and Orion Pharma (Finland), and speakers fee from Getinge (Sweden). Dr. de Man disclosed the off-label product use of oxidation-reduction potential measurement with the RedoxSYS System from Aytu Biosciences. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Proof of Concept, Feasibility, and Efficacy Trials.Crit Care Med. 2022 Sep 1;50(9):e731-e732. doi: 10.1097/CCM.0000000000005581. Epub 2022 Aug 15. Crit Care Med. 2022. PMID: 35984068 No abstract available.
References
-
- Goligher EC, Dres M, Fan E, et al. : Mechanical ventilation–induced diaphragm atrophy strongly impacts clinical outcomes. Am J Respir Crit Care Med. 2018; 197:204–213 - PubMed
-
- Dres M, Dubé BP, Mayaux J, et al. : Coexistence and impact of limb muscle and diaphragm weakness at time of liberation from mechanical ventilation in medical intensive care unit patients. Am J Respir Crit Care Med. 2017; 195:57–66 - PubMed
-
- Dres M, Goligher EC, Heunks LMA, et al. : Critical illness-associated diaphragm weakness. Intensive Care Med. 2017; 43:1441–1452 - PubMed
-
- Levine S, Nguyen T, Taylor N, et al. : Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N Engl J Med. 2008; 358:1327–1335 - PubMed
-
- Goligher EC, Fan E, Herridge MS, et al. : Evolution of diaphragm thickness during mechanical ventilation. Impact of inspiratory effort. Am J Respir Crit Care Med. 2015; 192:1080–1088 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
