

The Utility of Cerebral Autoregulation Indices in Detecting Severe Brain Injury Varies by Cooling Treatment Phase in Neonates with Hypoxic-Ischemic Encephalopathy
- PMID: 35100588
- PMCID: PMC9828944
- DOI: 10.1159/000522314
The Utility of Cerebral Autoregulation Indices in Detecting Severe Brain Injury Varies by Cooling Treatment Phase in Neonates with Hypoxic-Ischemic Encephalopathy
Abstract
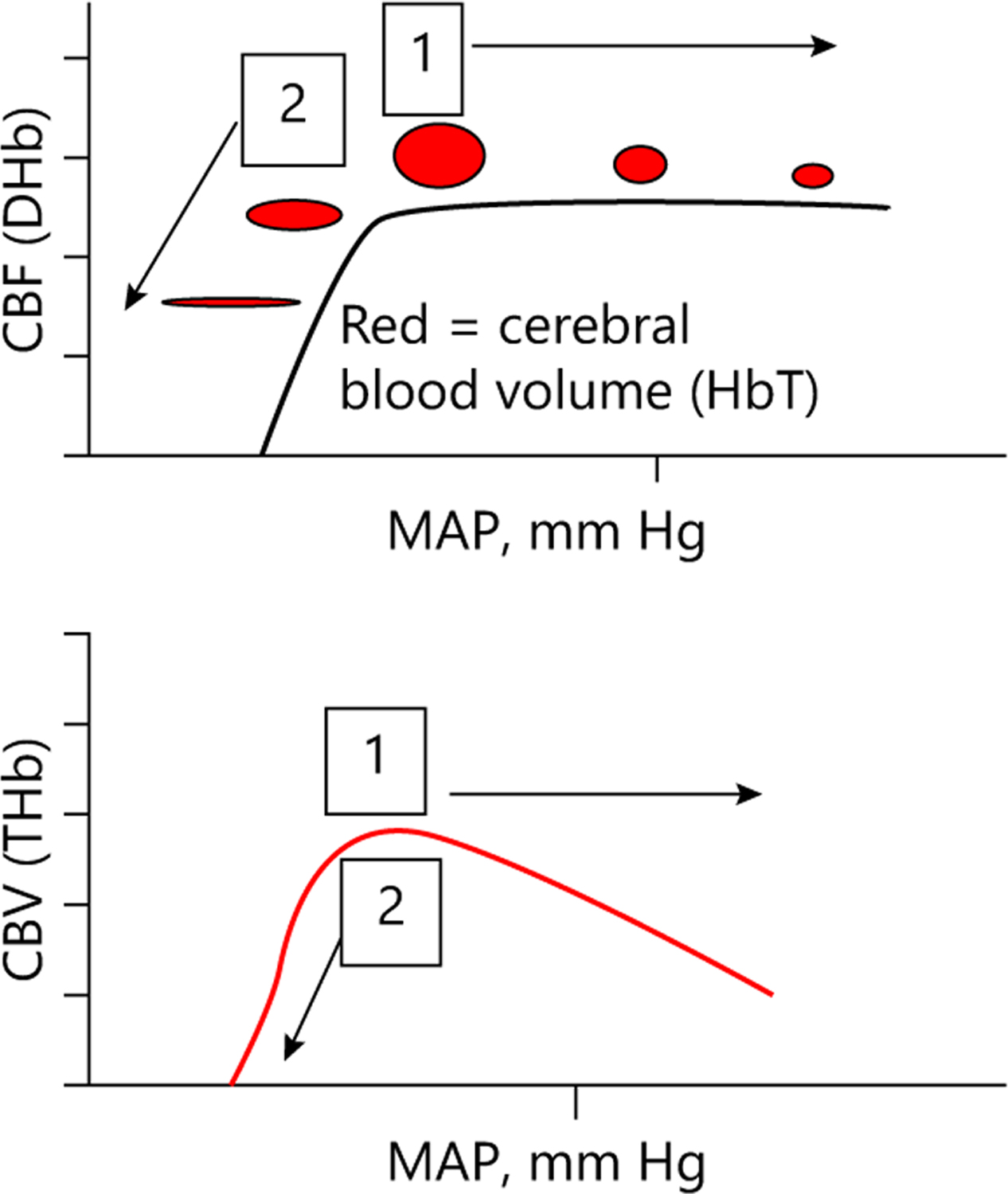
Identifying the hemodynamic range that best supports cerebral perfusion using near infrared spectroscopy (NIRS) autoregulation monitoring is a potential physiologic marker for neonatal hypoxic-ischemic encephalopathy (HIE) during therapeutic hypothermia. However, an optimal autoregulation monitoring algorithm has not been identified for neonatal clinical medicine. We tested whether the hemoglobin volume phase (HVP), hemoglobin volume (HVx), and pressure passivity index (PPI) identify changes in autoregulation that are associated with brain injury on MRI or death. The HVP measures the phase difference between a NIRS metric of cerebral blood volume, the total hemoglobin (THb), and mean arterial blood pressure (MAP) at the frequency of maximum coherence. The HVx is the correlation coefficient between MAP and THb. The PPI is the percentage of coherent MAP-DHb (difference between oxygenated and deoxygenated hemoglobin, a marker of cerebral blood flow) epochs in a chosen time period. Neonates cooled for HIE were prospectively enrolled in an observational study in two neonatal intensive care units. In analyses adjusted for study site and encephalopathy level, all indices detected relationships between poor autoregulation in the first 6 h after rewarming with a higher injury score on MRI. Only HVx and PPI during hypothermia and the PPI during rewarming identified autoregulatory dysfunction associated with a poor outcome independent of study site and encephalopathy level. Our findings suggest that the accuracy of mathematical autoregulation algorithms in detecting the risk of brain injury or death may depend on temperature and postnatal age. Extending autoregulation monitoring beyond the standard 72 h of therapeutic hypothermia may serve as a method to provide personalized care by assessing the need for and efficacy of future therapies after the hypothermia treatment phase.
Keywords: Brain injury; Cerebral autoregulation; Hypothermia; MRI; Near infrared spectroscopy; Neonatal hypoxia-ischemia.
© 2022 S. Karger AG, Basel.
Conflict of interest statement
Conflict of Interest Statement
Dr. Lee was previously a paid consultant for Medtronic and she is currently a paid consultant for Edwards Life Sciences. These arrangements have been reviewed and approved by the Johns Hopkins University in accordance with its conflict of interest policies. Medtronic and Edwards Life Sciences had no role in the design of the current study, collection or analysis of the data, interpretation of the results, manuscript writing, or our decision to submit this manuscript for publication.
Figures
References
-
- Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, et al. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015;385(9966): 430–40. - PubMed
-
- Shankaran S, Laptook AR, Ehrenkranz RA, Tyson JE, McDonald SA, Donovan EF, et al. Whole-body hypothermia for neonates with hypoxic–ischemic encephalopathy. N Engl J Med. 2005;353(15):1574–84. - PubMed
-
- Azzopardi D, Strohm B, Marlow N, Brocklehurst P, Deierl A, Eddama O, et al. Effects of hypothermia for perinatal asphyxia on childhood outcomes. N Engl J Med. 2014;371(2): 140–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
