

Does surgical technique influence the burden of lung metastases in patients with pathologic long bone fractures?
- PMID: 35101024
- PMCID: PMC8802478
- DOI: 10.1186/s12891-022-05067-5
Does surgical technique influence the burden of lung metastases in patients with pathologic long bone fractures?
Abstract
Background: The aims of this study are to (1) determine whether fixation of metastatic long bone fractures with an intramedullary nail (IMN) influences the incidence of lung metastasis in comparison to arthroplasty or ORIF (Arthro/ORIF); and (2) assess this relationship in primary tumor types; and (3) to assess survival implications of lung metastasis after surgery.
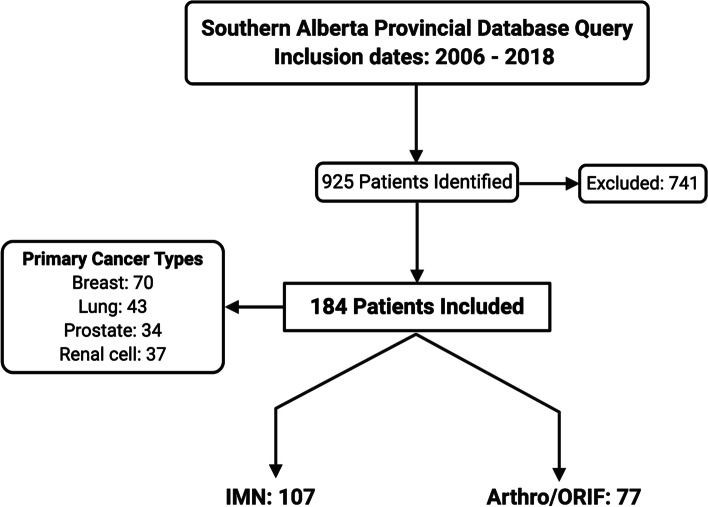
Methods: Retrospective cohort study investigating 184 patients (107 IMN, and 77 Arthro/ORIF) surgically treated for metastatic long bone fractures. Patients were required to have a single surgically treated impending or established pathologic fracture of a long bone, pre-operative lung imaging (lung radiograph or computed tomography) and post-operative lung imaging within 6 months of surgery. Primary cancer types included were breast (n = 70), lung (n = 43), prostate (n = 34), renal cell (n = 37). Statistical analyses were conducted using two-tailed Fisher's exact tests, and Kaplan-Meier survival analyses.
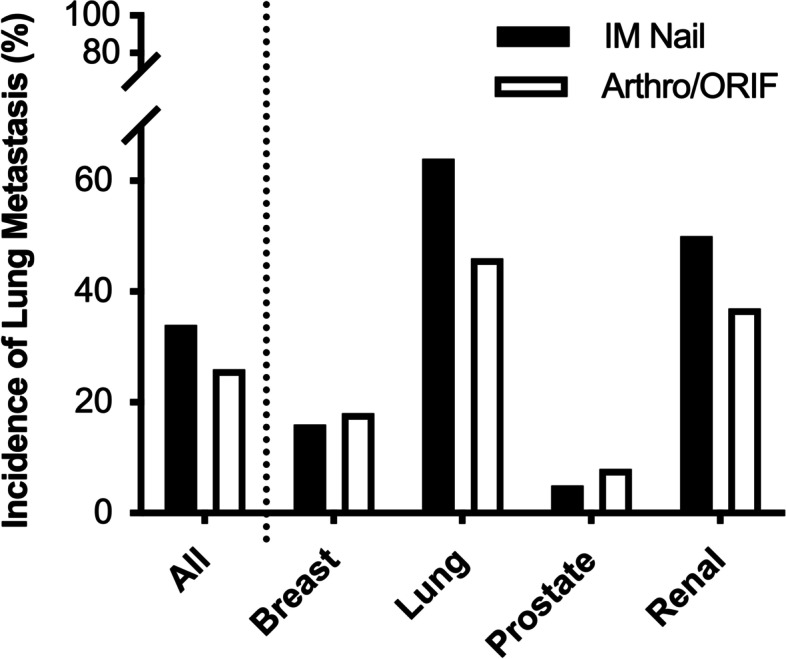
Results: Patients treated with IMN and Arthro/ORIF developed new or progressive lung metastases following surgery at an incidence of 34 and 26%, respectively. Surgical method did not significantly influence lung metastasis (p = 0.33). Furthermore, an analysis of primary cancer subgroups did not yield any differences between IMN vs Arthro/ORIF. Median survival for the entire cohort was 11 months and 1-year overall survival was 42.7% (95% CI: 35.4-49.8). Regardless of fixation method, the presence of new or progressive lung metastatic disease at follow up imaging study was found to have a negative impact on patient survival (p < 0.001).
Conclusions: In this study, development or progression of metastatic lung disease was not affected by long bone stabilization strategy. IM manipulation of metastatic long bone fractures therefore may not result in a clinically relevant increase in metastatic lung burden. The results of this study also suggest that lung metastasis within 6 months of surgery for metastatic long bone lesions is negatively associated with patient survival.
Level of evidence: III, therapeutic study.
Keywords: Arthroplasty; Intramedullary nail; Lung metastasis; Metastatic bone disease; Pathologic fracture.
© 2022. The Author(s).
Conflict of interest statement
No competing interests for all authors.
Figures


References
-
- Jemal A, Ward EM, Johnson CJ, Cronin KA, Ma J, Ryerson B, Mariotto A, Lake AJ, Wilson R, Sherman RL, Anderson RN, Henley SJ, Kohler BA, Penberthy L, Feuer EJ, Weir HK. Annual Report to the Nation on the Status of Cancer, 1975–2014, Featuring Survival. J Natl Cancer Inst. 2017;109(9):djx030. doi: 10.1093/jnci/djx030. - DOI - PMC - PubMed
-
- Ratasvuori M, Wedin R, Keller J, Nottrott M, Zaikova O, Bergh P, Kalen A, Nilsson J, Jonsson H, Laitinen M. Insight opinion to surgically treated metastatic bone disease: Scandinavian sarcoma group skeletal metastasis registry report of 1195 operated skeletal metastasis. Surg Oncol. 2013;22(2):132–138. doi: 10.1016/j.suronc.2013.02.008. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
