

Multicentre analysis of practice patterns regarding benzodiazepine use in cardiac surgery
- PMID: 35101244
- PMCID: PMC9074791
- DOI: 10.1016/j.bja.2021.11.040
Multicentre analysis of practice patterns regarding benzodiazepine use in cardiac surgery
Abstract
Background: There is controversy regarding optimal use of benzodiazepines during cardiac surgery, and it is unknown whether and to what extent there is variation in practice. We sought to describe benzodiazepine use and sources of variation during cardiac surgeries across patients, clinicians, and institutions.
Methods: We conducted an analysis of adult cardiac surgeries across a multicentre consortium of USA academic and private hospitals from 2014 to 2019. The primary outcome was administration of a benzodiazepine from 2 h before anaesthesia start until anaesthesia end. Institutional-, clinician-, and patient-level variables were analysed via multilevel mixed-effects models.
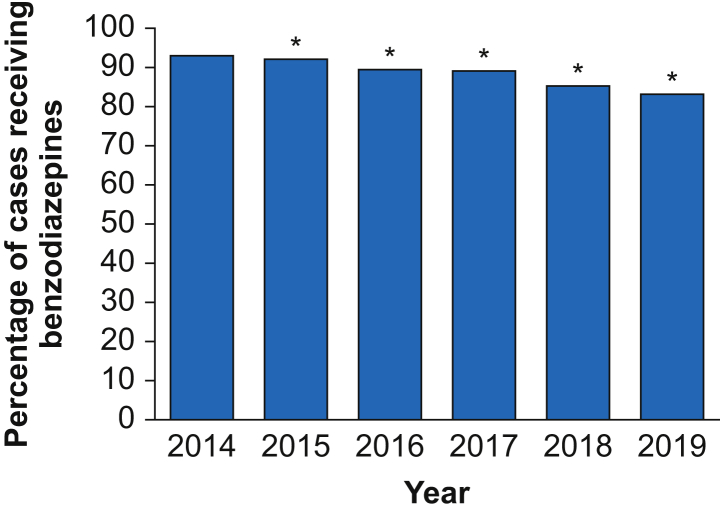
Results: Of 65 508 patients cared for by 825 anaesthesiology attending clinicians (consultants) at 33 institutions, 58 004 patients (88.5%) received benzodiazepines with a median midazolam-equivalent dose of 4.0 mg (inter-quartile range [IQR], 2.0-6.0 mg). Variation in benzodiazepine dosage administration was 54.7% attributable to institution, 14.7% to primary attending anaesthesiology clinician, and 30.5% to patient factors. The adjusted median odds ratio for two similar patients receiving a benzodiazepine was 2.68 between two randomly selected clinicians and 4.19 between two randomly selected institutions. Factors strongly associated (adjusted odds ratio, <0.75, or >1.25) with significantly decreased likelihoods of benzodiazepine administration included older age (>80 vs ≤50 yr; adjusted odds ratio=0.04; 95% CI, 0.04-0.05), university affiliation (0.08, 0.02-0.35), recent year of surgery (0.42, 0.37-0.49), and low clinician case volume (0.44, 0.25-0.75). Factors strongly associated with significantly increased likelihoods of benzodiazepine administration included cardiopulmonary bypass (2.26, 1.99-2.55), and drug use history (1.29, 1.02-1.65).
Conclusions: Two-thirds of the variation in benzodiazepine administration during cardiac surgery are associated with institutions and attending anaesthesiology clinicians (consultants). These data, showing wide variations in administration, suggest that rigorous research is needed to guide evidence-based and patient-centred benzodiazepine administration.
Keywords: anaesthesia; benzodiazepines; cardiac procedures; cardiovascular surgery; physicians; practice patterns.
Copyright © 2021 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Figures



References
-
- Spence J., Belley-Côté E., Devereaux P.J., et al. Benzodiazepine administration during adult cardiac surgery: a survey of current practice among Canadian anesthesiologists working in academic centres. Can J Anaesth. 2018;65:263–271. - PubMed
-
- Spence J., Belley-Côté E., Lee S.F., et al. The role of randomized cluster crossover trials for comparative effectiveness testing in anesthesia: design of the Benzodiazepine-Free Cardiac Anesthesia for Reduction in Postoperative Delirium (B-Free) trial. Can J Anaesth. 2018;65:813–821. - PubMed
-
- Sebel P.S., Bowdle T.A., Ghoneim M.M., et al. The incidence of awareness during anesthesia: a multicenter United States study. Anesth Analg. 2004;99:833–839. table of contents. - PubMed
-
- American Society of Anesthesiologists Task Force on Intraoperative Awareness Practice advisory for intraoperative awareness and brain function monitoring: a report by the American Society of Anesthesiologists task force on intraoperative awareness. Anesthesiology. 2006;104:847–864. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
