

The history of ion beam therapy in Germany
- PMID: 35101337
- PMCID: PMC9948864
- DOI: 10.1016/j.zemedi.2021.11.003
The history of ion beam therapy in Germany
Abstract
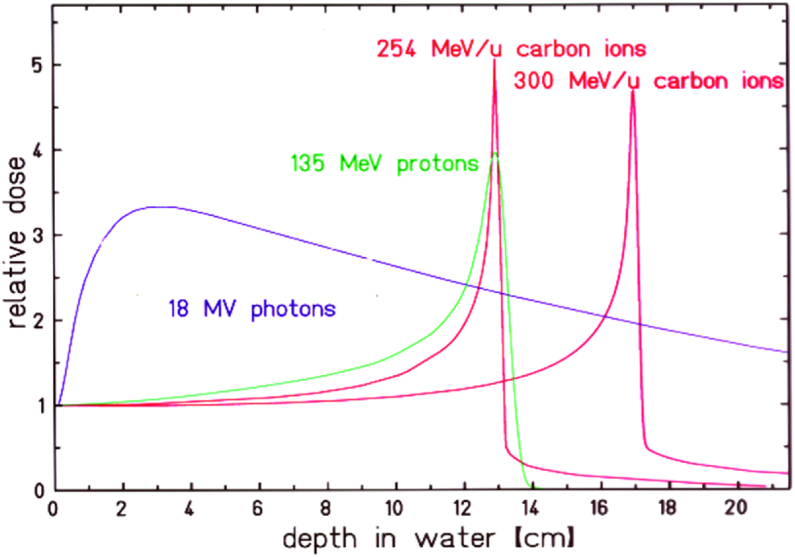
The advantageous depth dose profile of ion beams together with state of the art beam delivery and treatment planning systems allow for highly conformal tumor treatments in patients. First treatments date back to 1954 at the Lawrence Berkeley Laboratory (LBL) and in Europe, ion beam therapy started in the mid-1990s at the Paul-Scherrer Institute (PSI) with protons and at the Helmholtz Center for Heavy Ion Research (GSI) with carbon ions, followed by the Heidelberg Ion Therapy Center (HIT) in Heidelberg. This review describes the historical development of ion beam therapy in Germany based on the pioneering work at LBL and in the context of simultaneous developments in other countries as well as recent developments.
Keywords: Beam scanning; Carbon ion therapy; Light ion beam therapy; Relative biological effectiveness.
Copyright © 2021. Published by Elsevier GmbH.
Figures








References
-
- Wilson R.R. Radiological use of fast protons. Radiology. 1946;47(5):487–491. - PubMed
-
- Bethge K., Kreisler K.G.P., Walter G. Springer; Heidelberg: 2004. Hadron therapy in medical applications of nuclear physics.
-
- Tobias C., et al. Pituitary irradiation with high-energy proton beams a preliminary report. Cancer Res. 1958;18(2):121–134. - PubMed
-
- Linstadt D.E., Castro J.R., Phillips T.L. Neon ion radiotherapy: results of the phase I/II clinical trial. Int J Radiat Oncol Biol Phys. 1991;20(4):761–769. - PubMed
-
- Larsson B. Pre-therapeutic physical experiments with high energy protons. Br J Radiol. 1961;34(399):143–151. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
