

Outcomes in patients with and without disability admitted to hospital with COVID-19: a retrospective cohort study
- PMID: 35101870
- PMCID: PMC8900770
- DOI: 10.1503/cmaj.211277
Outcomes in patients with and without disability admitted to hospital with COVID-19: a retrospective cohort study
Erratum in
-
Correction to "Outcomes in patients with and without disability admitted to hospital with COVID-19: a retrospective cohort study".CMAJ. 2022 Jul 11;194(26):E916. doi: 10.1503/cmaj.220925. CMAJ. 2022. PMID: 35817436 Free PMC article. No abstract available.
Abstract
Background: Disability-related considerations have largely been absent from the COVID-19 response, despite evidence that people with disabilities are at elevated risk for acquiring COVID-19. We evaluated clinical outcomes in patients who were admitted to hospital with COVID-19 with a disability compared with patients without a disability.
Methods: We conducted a retrospective cohort study that included adults with COVID-19 who were admitted to hospital and discharged between Jan. 1, 2020, and Nov. 30, 2020, at 7 hospitals in Ontario, Canada. We compared in-hospital death, admission to the intensive care unit (ICU), hospital length of stay and unplanned 30-day readmission among patients with and without a physical disability, hearing or vision impairment, traumatic brain injury, or intellectual or developmental disability, overall and stratified by age (≤ 64 and ≥ 65 yr) using multivariable regression, controlling for sex, residence in a long-term care facility and comorbidity.
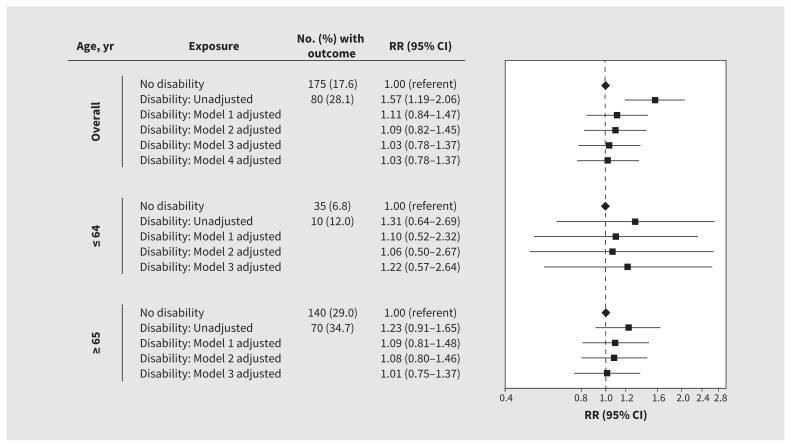
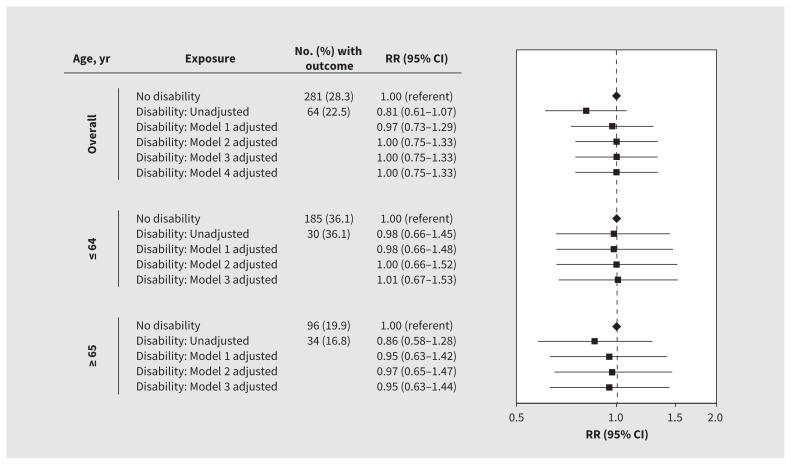
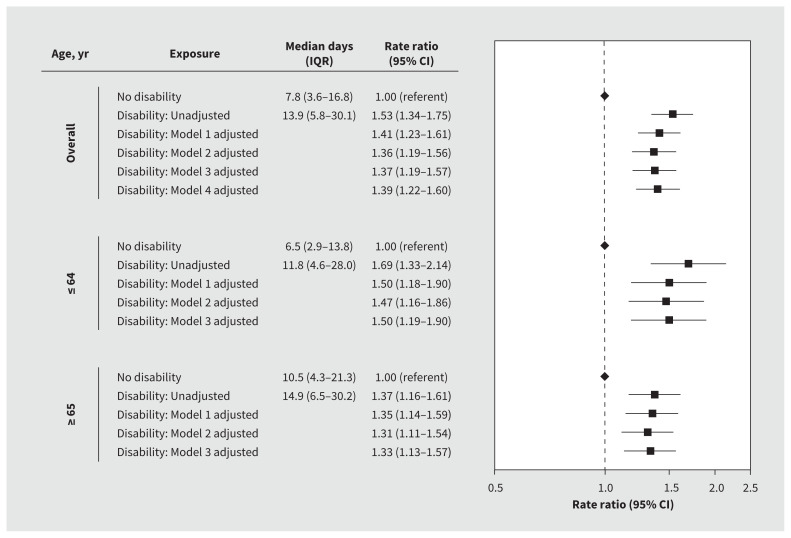
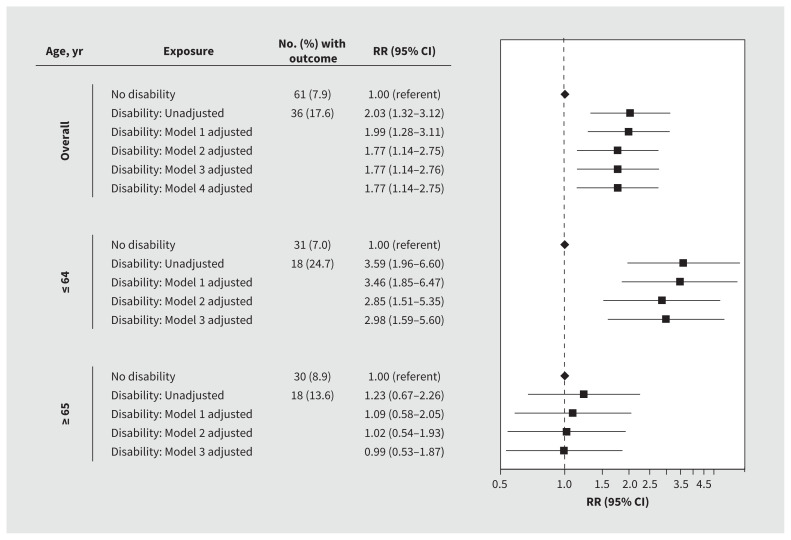
Results: Among 1279 admissions to hospital for COVID-19, 22.3% had a disability. We found that patients with a disability were more likely to die than those without a disability (28.1% v. 17.6%), had longer hospital stays (median 13.9 v. 7.8 d) and more readmissions (17.6% v. 7.9%), but had lower ICU admission rates (22.5% v. 28.3%). After adjustment, there were no statistically significant differences between those with and without disabilities for in-hospital death or admission to ICU. After adjustment, patients with a disability had longer hospital stays (rate ratio 1.36, 95% confidence interval [CI] 1.19-1.56) and greater risk of readmission (relative risk 1.77, 95% CI 1.14-2.75). In age-stratified analyses, we observed longer hospital stays among patients with a disability than in those without, in both younger and older subgroups; readmission risk was driven by younger patients with a disability.
Interpretation: Patients with a disability who were admitted to hospital with COVID-19 had longer stays and elevated readmission risk than those without disabilities. Disability-related needs should be addressed to support these patients in hospital and after discharge.
© 2022 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests: Amol Verma has received personal fees from Ontario Health, and personal grant funding from AMS Healthcare (Compassion and AI Fellowship) and St. Michael’s Hospital. Michael Fralick is a consultant for Proof Diagnostics, a company that has created a point-of-care testing device using CRISPR for COVID-19. He has also received grants from the Canadian Institutes of Health Research (CIHR) and support from grants from the Canadian Military for clinical trials to identify treatments for COVID-19. Fahad Razak has received personal fees from Ontario Health and is a member of the Ontario COVID-19 Science Advisory Table. Yona Lunsky has received a grant from CIHR for research on disability and health during COVID-19. She is a member of the Board of Directors for Special Olympics Canada. Margaret Herridge has received grants from CIHR. No other competing interests were declared.
Figures
References
-
- World report on disability. Geneva: World Health Organization; 2011. - PubMed