

Equitable access to COVID-19 vaccines makes a life-saving difference to all countries
- PMID: 35102361
- PMCID: PMC8873023
- DOI: 10.1038/s41562-022-01289-8
Equitable access to COVID-19 vaccines makes a life-saving difference to all countries
Abstract
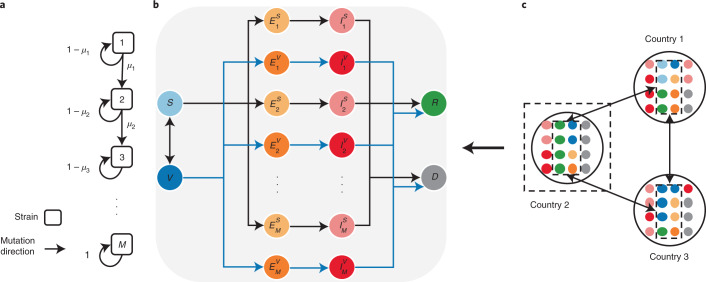
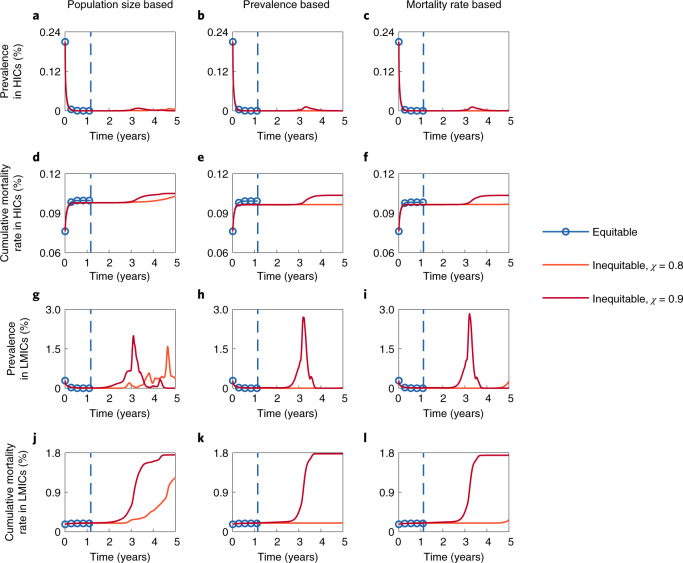
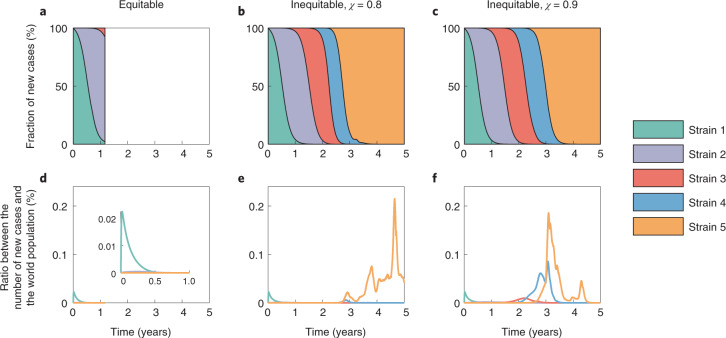
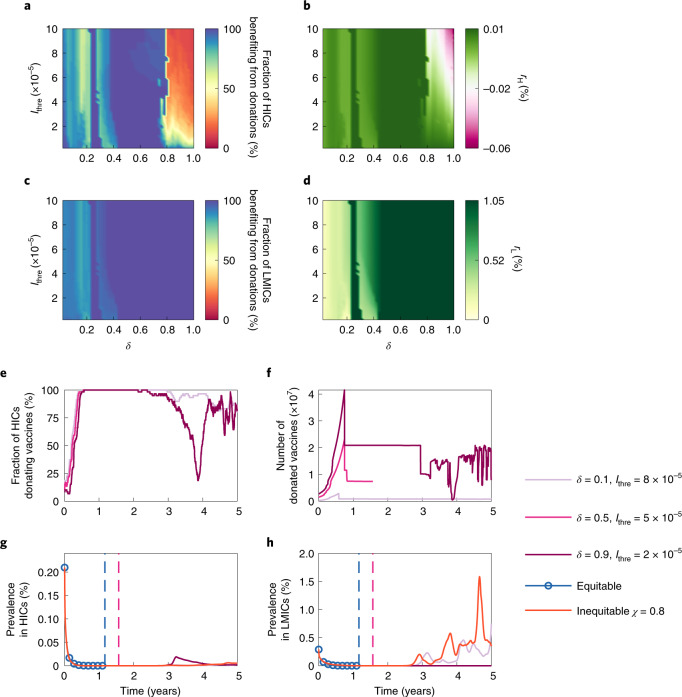
Despite broad agreement on the negative consequences of vaccine inequity, the distribution of COVID-19 vaccines is imbalanced. Access to vaccines in high-income countries (HICs) is far greater than in low- and middle-income countries (LMICs). As a result, there continue to be high rates of COVID-19 infections and deaths in LMICs. In addition, recent mutant COVID-19 outbreaks may counteract advances in epidemic control and economic recovery in HICs. To explore the consequences of vaccine (in)equity in the face of evolving COVID-19 strains, we examine vaccine allocation strategies using a multistrain metapopulation model. Our results show that vaccine inequity provides only limited and short-term benefits to HICs. Sharper disparities in vaccine allocation between HICs and LMICs lead to earlier and larger outbreaks of new waves. Equitable vaccine allocation strategies, in contrast, substantially curb the spread of new strains. For HICs, making immediate and generous vaccine donations to LMICs is a practical pathway to protect everyone.
© 2022. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Vaccine inequality benefits no one.Nat Hum Behav. 2022 Feb;6(2):177-178. doi: 10.1038/s41562-022-01297-8. Nat Hum Behav. 2022. PMID: 35102352 No abstract available.
References
-
- WHO Coronavirus Disease (COVID-19) Dashboard (World Health Organization, 2021); https://covid19.who.int/
-
- The COVID-19 Candidate Vaccine Landscape and Tracker (World Health Organization, 2021); https://www.who.int/publications/m/item/draft-landscape-of-covid-19-cand...
-
- Mathieu E, et al. A global database of COVID-19 vaccinations. Nat. Hum. Behav. 2021;5:947–953. - PubMed
-
- Bollyky TJ, Gostin LO, Hamburg MA. The equitable distribution of COVID-19 therapeutics and vaccines. JAMA. 2020;323:2462–2463. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- C7154-20GF/Research Grants Council, University Grants Committee (RGC, UGC)
- C7151-20GF/Research Grants Council, University Grants Committee (RGC, UGC)
- C1143-20GF/Research Grants Council, University Grants Committee (RGC, UGC)
- COVID190215/Food and Health Bureau of the Government of the Hong Kong Special Administrative Region | Health and Medical Research Fund (HMRF)
LinkOut - more resources
Full Text Sources
Medical
