

Quantifying longitudinal cognitive resilience to Alzheimer's disease and other neuropathologies
- PMID: 35102704
- PMCID: PMC10119432
- DOI: 10.1002/alz.12576
Quantifying longitudinal cognitive resilience to Alzheimer's disease and other neuropathologies
Abstract
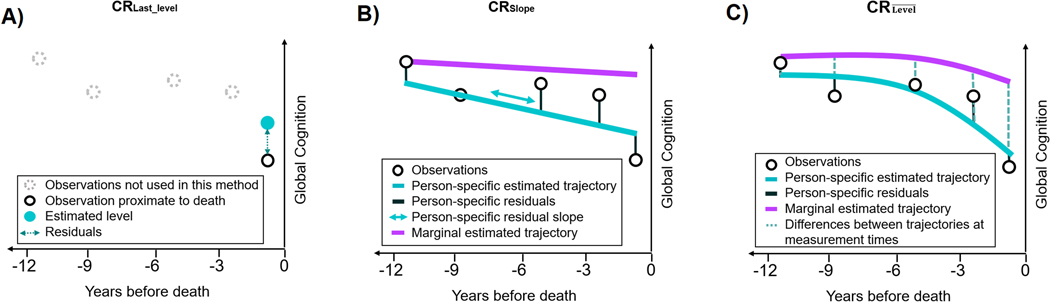
Introduction: Cognitive resilience (CR) has been defined as the continuum of better (or worse) than expected cognition, given the degree of neuropathology. To quantify this concept, existing approaches focus on either cognitive level at a single time point or slopes of cognitive decline.
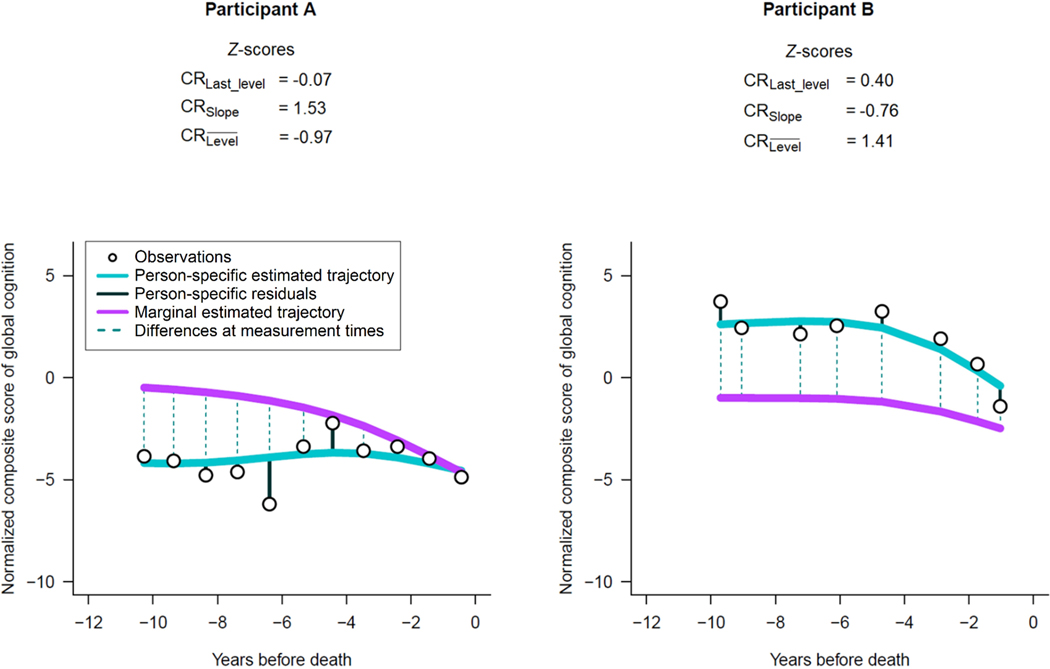
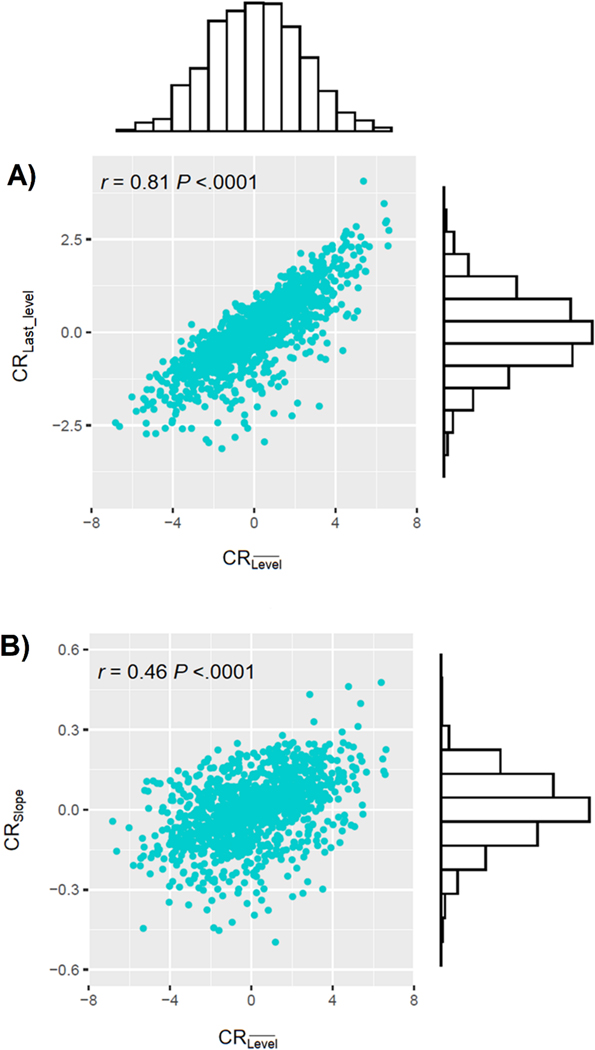
Methods: In a prospective study of 1215 participants, we created a continuous measure of CR defined as the mean of differences between estimated person-specific and marginal cognitive levels over time, after accounting for neuropathologies.
Results: Neuroticism and depressive symptoms were associated with all CR measures (P-values < .012); as expected, cognitive activity and education were only associated with the cognitive-level approaches (P-values < .0002). However, compared with the existing CR measures focusing on a single measure or slopes of cognition, our new measure yielded stronger relations with risk factors.
Discussion: Defining CR based on the longitudinal differences between person-specific and marginal cognitive levels is a novel and complementary way to quantify CR.
Keywords: Alzheimer's dementia; cognitive resilience; longitudinal study; mixed-effects model; neuropathology; neuropsychological tests.
© 2022 the Alzheimer's Association.
Conflict of interest statement
Conflicts of interest
The authors have no conflicts to declare.
Figures
Similar articles
-
The association of MIND diet with cognitive resilience to neuropathologies.Alzheimers Dement. 2023 Aug;19(8):3644-3653. doi: 10.1002/alz.12982. Epub 2023 Feb 28. Alzheimers Dement. 2023. PMID: 36855023 Free PMC article.
-
Quantifying cognitive resilience in Alzheimer's Disease: The Alzheimer's Disease Cognitive Resilience Score.PLoS One. 2020 Nov 5;15(11):e0241707. doi: 10.1371/journal.pone.0241707. eCollection 2020. PLoS One. 2020. PMID: 33152028 Free PMC article.
-
Person-specific contribution of neuropathologies to cognitive loss in old age.Ann Neurol. 2018 Jan;83(1):74-83. doi: 10.1002/ana.25123. Epub 2018 Jan 14. Ann Neurol. 2018. PMID: 29244218 Free PMC article.
-
Structural magnetic resonance imaging for the early diagnosis of dementia due to Alzheimer's disease in people with mild cognitive impairment.Cochrane Database Syst Rev. 2020 Mar 2;3(3):CD009628. doi: 10.1002/14651858.CD009628.pub2. Cochrane Database Syst Rev. 2020. PMID: 32119112 Free PMC article.
-
The concept of resilience to Alzheimer's Disease: current definitions and cellular and molecular mechanisms.Mol Neurodegener. 2024 Apr 8;19(1):33. doi: 10.1186/s13024-024-00719-7. Mol Neurodegener. 2024. PMID: 38589893 Free PMC article. Review.
Cited by
-
Alzheimer's therapeutic development: shifting neurodegeneration to neuroregeneration.Trends Pharmacol Sci. 2024 Mar;45(3):197-209. doi: 10.1016/j.tips.2024.01.012. Epub 2024 Feb 14. Trends Pharmacol Sci. 2024. PMID: 38360510 Free PMC article. Review.
-
Sex differences in the executive and behavioral reserve of autosomal dominant frontotemporal dementia.Alzheimers Dement. 2025 Apr;21(4):e70070. doi: 10.1002/alz.70070. Alzheimers Dement. 2025. PMID: 40277045 Free PMC article.
-
The association of MIND diet with cognitive resilience to neuropathologies.Alzheimers Dement. 2023 Aug;19(8):3644-3653. doi: 10.1002/alz.12982. Epub 2023 Feb 28. Alzheimers Dement. 2023. PMID: 36855023 Free PMC article.
-
Associations Between Loneliness and Cognitive Resilience to Neuropathology in Older Adults.J Gerontol B Psychol Sci Soc Sci. 2023 May 26;78(6):939-947. doi: 10.1093/geronb/gbad023. J Gerontol B Psychol Sci Soc Sci. 2023. PMID: 36789449 Free PMC article.
-
Estimating dementia risk in an African American population using the DCTclock.Front Aging Neurosci. 2024 Jan 11;15:1328333. doi: 10.3389/fnagi.2023.1328333. eCollection 2023. Front Aging Neurosci. 2024. PMID: 38274984 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
