

Human papillomavirus infection and seroprevalence among female university students in Mexico
- PMID: 35103580
- PMCID: PMC8993084
- DOI: 10.1080/21645515.2022.2028514
Human papillomavirus infection and seroprevalence among female university students in Mexico
Abstract
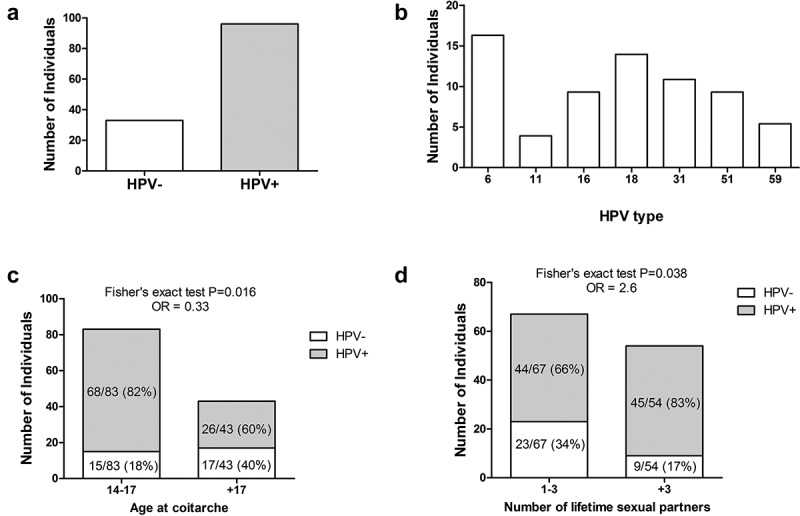
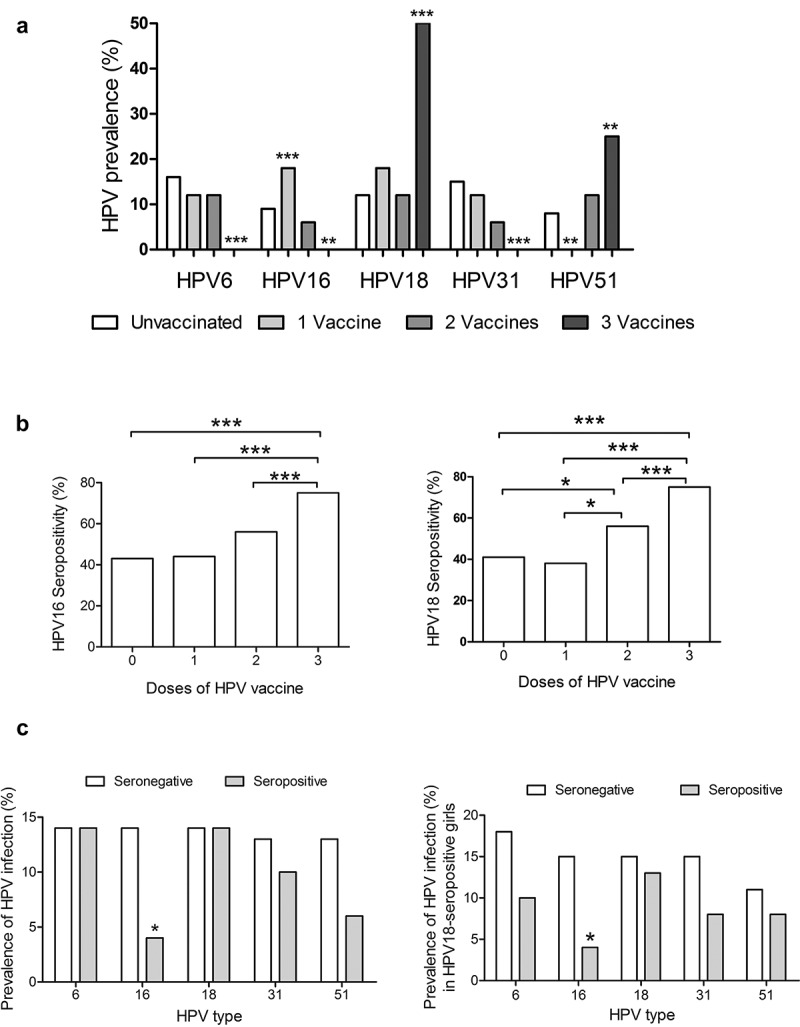
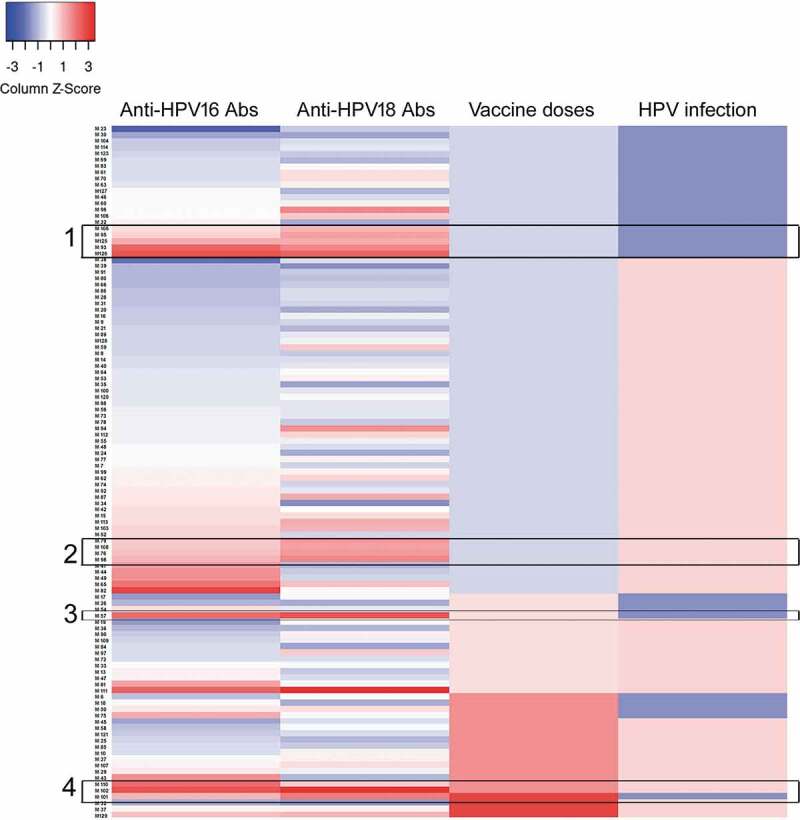
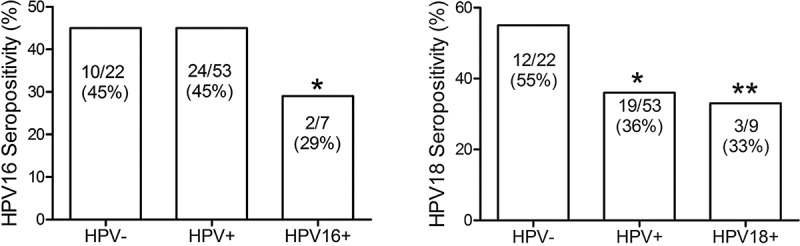
Human papillomavirus (HPV) is one of the most common causes of sexually transmitted diseases, and the main etiology of cervical cancer. This study was aimed to assess type-specific cervical HPV prevalence and their association with HPV-specific antibodies in a cohort of female university students. HPV genotyping was performed by amplifying and sequencing a fragment of the L1 protein. A BLAST search was performed to identify HPV types. HPV-specific IgG antibodies were measured by ELISA in serum samples. A total of 129 women participated, with an average age of 21.75 years. The prevalence of vaginal HPV infection was 74.42%. The most predominant high-risk HPV types were 18 (13.95%), 31 (10.85%), and 16 (9.3%). We found that early age at coitarche and a higher number of sexual partners were significantly associated with a high prevalence of HPV infection. In addition to sexual behavior, we observed that the presence of serum-specific IgG antibodies against HPV can impact the prevalence of the virus. Seropositivity to HPV-16 and HPV-18 was associated with a lower prevalence of HPV-16, but not for other HPV types. Of note, there was a lower proportion of HPV-specific seropositivity in women who had the presence of the same HPV type in a cervical specimen, suggesting an immunoregulatory mechanism associated with the viral infection. In conclusion, the prevalence of HPV in university women was higher than expected and it was associated with early age of sexual debut, an increasing number of sexual partners, and a low proportion of HPV seropositivity.
Keywords: Human papilloma virus; México; cervical cancer; prophylactic HPV vaccination; seroprevalence.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
-
- Aguilar-Lemarroy A, Vallejo-Ruiz V, Cortes-Gutierrez EI, Salgado-Bernabe ME, Ramos-Gonzalez NP, Ortega-Cervantes L, Arias‐Flores R, Medina‐Díaz IM, Hernández‐Garza F, Santos‐López G, Piña‐Sánchez P. Human papillomavirus infections in Mexican women with normal cytology, precancerous lesions, and cervical cancer: type-specific prevalence and HPV coinfections. J Med Virol. 2015;87:871–84. doi: 10.1002/jmv.24099. - DOI - PubMed
-
- Boda D, Docea AO, Calina D, Ilie MA, Caruntu C, Zurac S, Neagu M, Constantin C, Branisteanu DE, Voiculescu V, et al. Human papilloma virus: apprehending the link with carcinogenesis and unveiling new research avenues (Review). Int J Oncol. 2018;52:637–55. doi: 10.3892/ijo.2018.4256. - DOI - PMC - PubMed
-
- Walboomers JM, Jacobs MV, Manos MM, Bosch FX, Kummer JA, Shah KV, Snijders PJF, Peto J, Meijer CJLM, Muñoz N, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol. 1999;189:12–19. doi: 10.1002/(SICI)1096-9896(199909)189:1<12::AID-PATH431>3.0.CO;2-F. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials