

Effect of Moderate Hypothermia vs Normothermia on 30-Day Mortality in Patients With Cardiogenic Shock Receiving Venoarterial Extracorporeal Membrane Oxygenation: A Randomized Clinical Trial
- PMID: 35103766
- PMCID: PMC8808325
- DOI: 10.1001/jama.2021.24776
Effect of Moderate Hypothermia vs Normothermia on 30-Day Mortality in Patients With Cardiogenic Shock Receiving Venoarterial Extracorporeal Membrane Oxygenation: A Randomized Clinical Trial
Erratum in
-
Errors in Secondary Outcomes.JAMA. 2023 Apr 11;329(14):1226. doi: 10.1001/jama.2023.3806. JAMA. 2023. PMID: 37039807 Free PMC article. No abstract available.
Abstract
Importance: The optimal approach to the use of venoarterial extracorporeal membrane oxygenation (ECMO) during cardiogenic shock is uncertain.
Objective: To determine whether early use of moderate hypothermia (33-34 °C) compared with strict normothermia (36-37 °C) improves mortality in patients with cardiogenic shock receiving venoarterial ECMO.
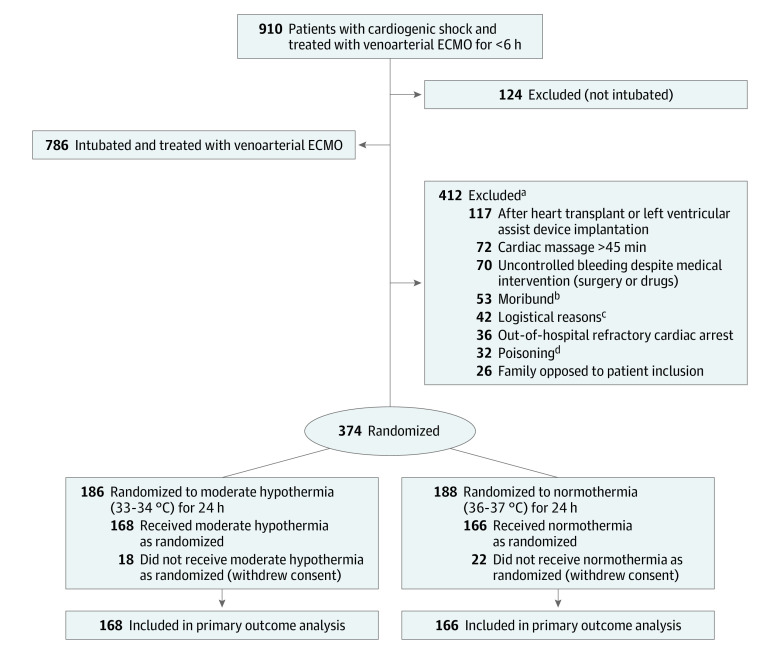
Design, setting, and participants: Randomized clinical trial of patients (who were eligible if they had been endotracheally intubated and were receiving venoarterial ECMO for cardiogenic shock for <6 hours) conducted in the intensive care units at 20 French cardiac shock care centers between October 2016 and July 2019. Of 786 eligible patients, 374 were randomized. Final follow-up occurred in November 2019.
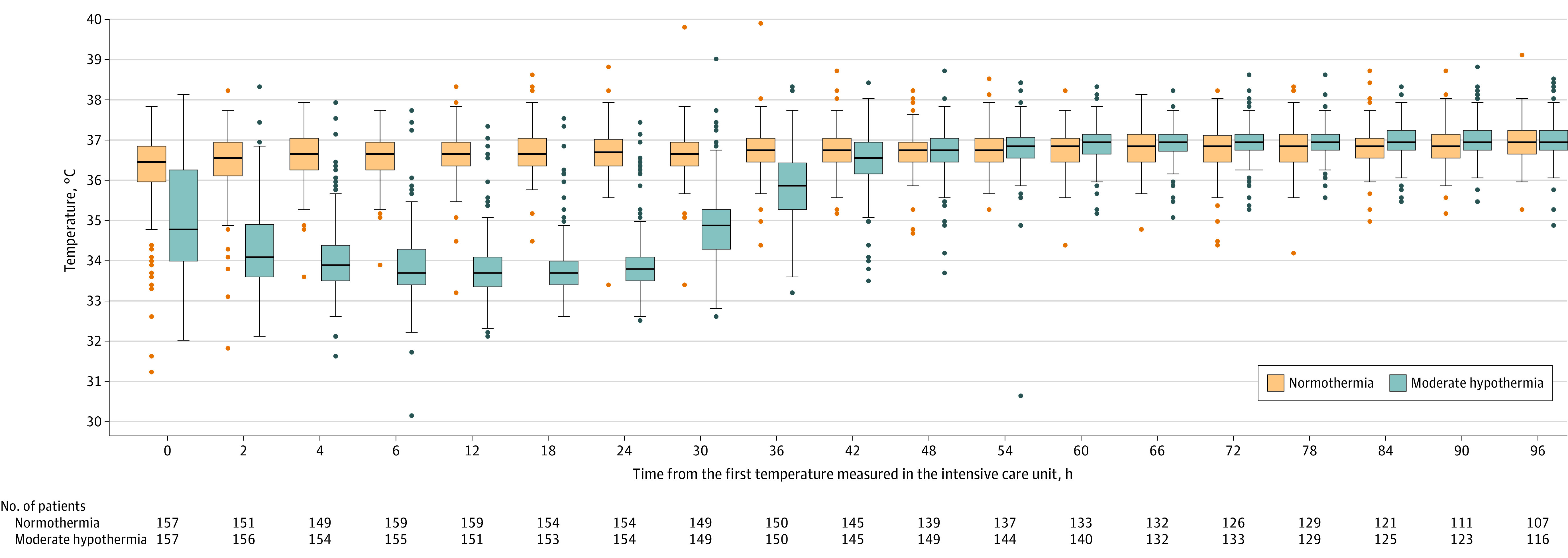
Interventions: Early moderate hypothermia (33-34 °C; n = 168) for 24 hours or strict normothermia (36-37 °C; n = 166).
Main outcomes and measures: The primary outcome was mortality at 30 days. There were 31 secondary outcomes including mortality at days 7, 60, and 180; a composite outcome of death, heart transplant, escalation to left ventricular assist device implantation, or stroke at days 30, 60, and 180; and days without requiring a ventilator or kidney replacement therapy at days 30, 60, and 180. Adverse events included rates of severe bleeding, sepsis, and number of units of packed red blood cells transfused during venoarterial ECMO.
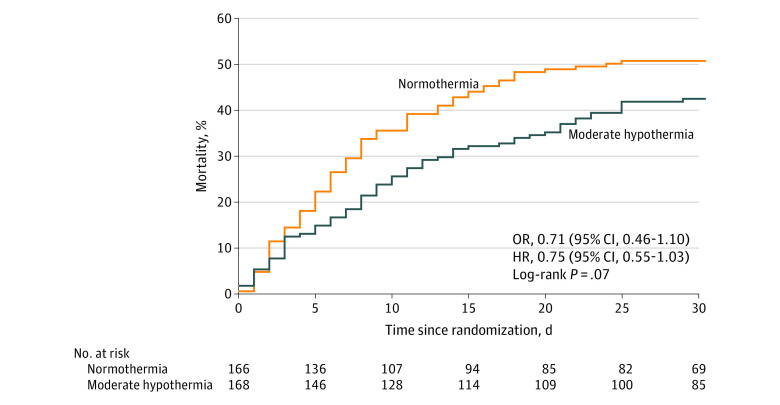
Results: Among the 374 patients who were randomized, 334 completed the trial (mean age, 58 [SD, 12] years; 24% women) and were included in the primary analysis. At 30 days, 71 patients (42%) in the moderate hypothermia group had died vs 84 patients (51%) in the normothermia group (adjusted odds ratio, 0.71 [95% CI, 0.45 to 1.13], P = .15; risk difference, -8.3% [95% CI, -16.3% to -0.3%]). For the composite outcome of death, heart transplant, escalation to left ventricular assist device implantation, or stroke at day 30, the adjusted odds ratio was 0.61 (95% CI, 0.39 to 0.96; P = .03) for the moderate hypothermia group compared with the normothermia group and the risk difference was -11.5% (95% CI, -23.2% to 0.2%). Of the 31 secondary outcomes, 30 were inconclusive. The incidence of moderate or severe bleeding was 41% in the moderate hypothermia group vs 42% in the normothermia group. The incidence of infections was 52% in both groups. The incidence of bacteremia was 20% in the moderate hypothermia group vs 30% in the normothermia group.
Conclusions and relevance: In this randomized clinical trial involving patients with refractory cardiogenic shock treated with venoarterial ECMO, early application of moderate hypothermia for 24 hours did not significantly increase survival compared with normothermia. However, because the 95% CI was wide and included a potentially important effect size, these findings should be considered inconclusive.
Trial registration: ClinicalTrials.gov Identifier: NCT02754193.
Conflict of interest statement
Figures
Comment in
-
Moderate Hypothermia vs Normothermia and 30-Day Mortality in Patients With Cardiogenic Shock Receiving Venoarterial ECMO.JAMA. 2022 May 17;327(19):1927-1928. doi: 10.1001/jama.2022.5043. JAMA. 2022. PMID: 35579646 No abstract available.
-
Moderate Hypothermia vs Normothermia and 30-Day Mortality in Patients With Cardiogenic Shock Receiving Venoarterial ECMO.JAMA. 2022 May 17;327(19):1928. doi: 10.1001/jama.2022.5040. JAMA. 2022. PMID: 35579647 No abstract available.
-
Pharmacological and Nonpharmacological Supports in Shock.Am J Respir Crit Care Med. 2023 Jul 15;208(2):196-198. doi: 10.1164/rccm.202206-1165RR. Am J Respir Crit Care Med. 2023. PMID: 37141107 No abstract available.
