

Postoperative changes in cognition and cerebrospinal fluid neurodegenerative disease biomarkers
- PMID: 35104057
- PMCID: PMC8862419
- DOI: 10.1002/acn3.51499
Postoperative changes in cognition and cerebrospinal fluid neurodegenerative disease biomarkers
Abstract
Objective: Numerous investigators have theorized that postoperative changes in Alzheimer's disease neuropathology may underlie postoperative neurocognitive disorders. Thus, we determined the relationship between postoperative changes in cognition and cerebrospinal (CSF) tau, p-tau-181p, or Aβ levels after non-cardiac, non-neurologic surgery in older adults.
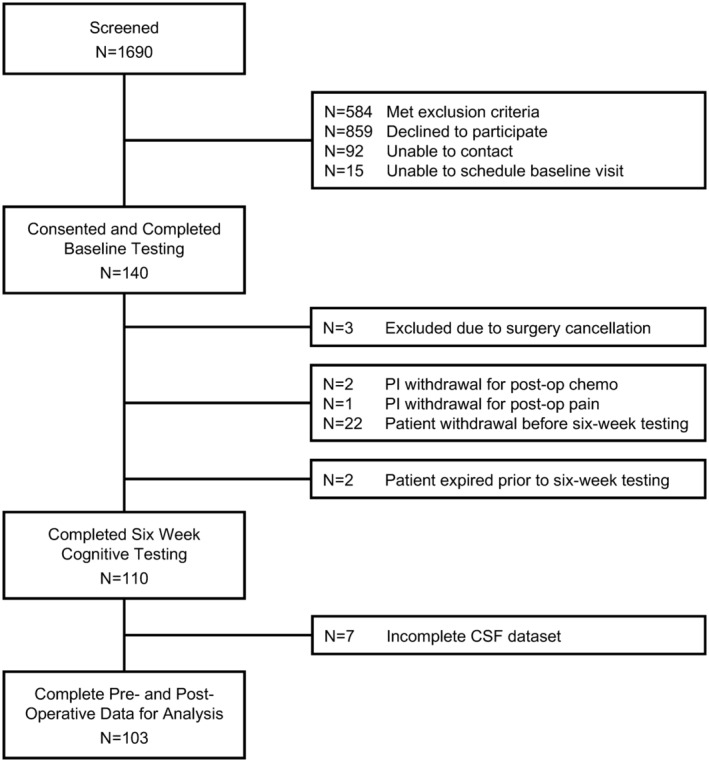
Methods: Participants underwent cognitive testing before and 6 weeks after surgery, and lumbar punctures before, 24 h after, and 6 weeks after surgery. Cognitive scores were combined via factor analysis into an overall cognitive index. In total, 110 patients returned for 6-week postoperative testing and were included in the analysis.
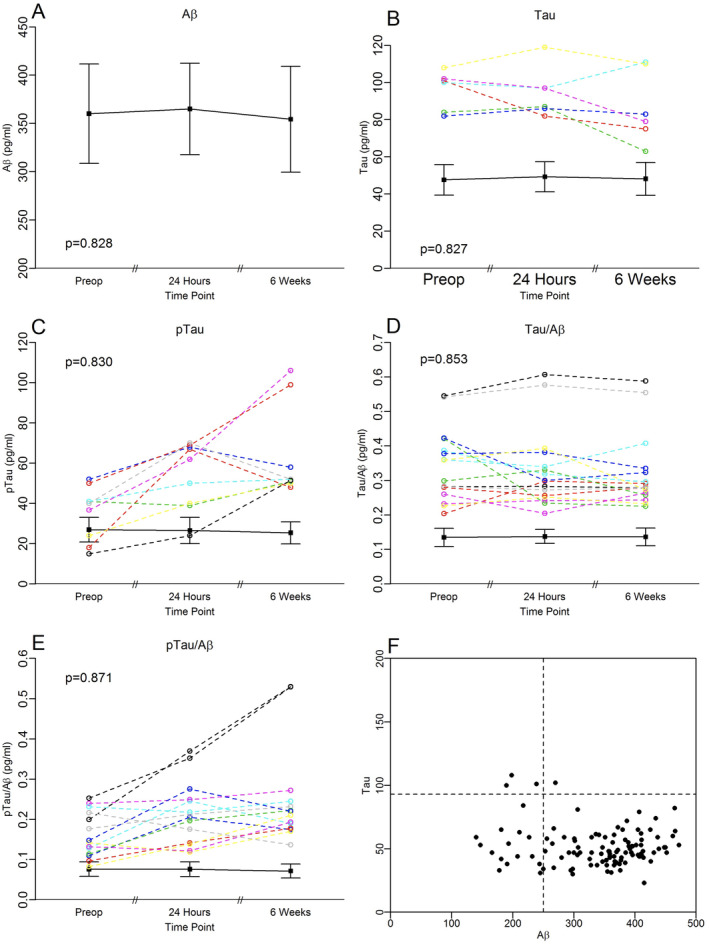
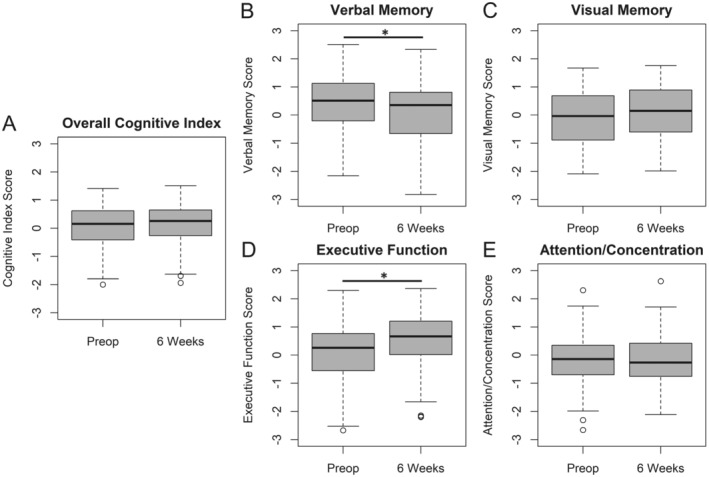
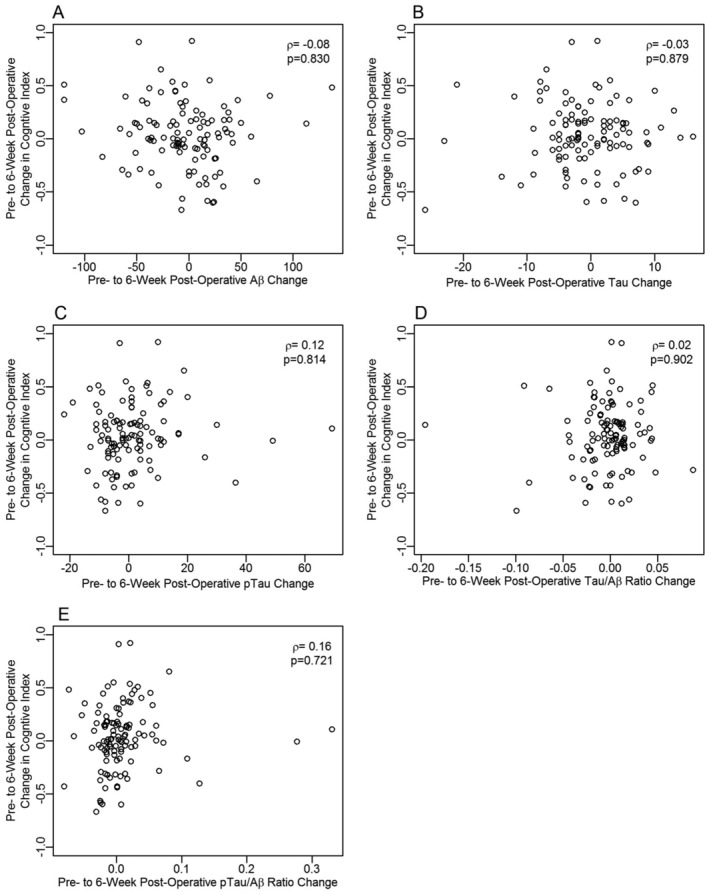
Results: There was no significant change from before to 24 h or 6 weeks following surgery in CSF tau (median [median absolute deviation] change before to 24 h: 0.00 [4.36] pg/mL, p = 0.853; change before to 6 weeks: -1.21 [3.98] pg/mL, p = 0.827). There were also no significant changes in CSF p-tau-181p or Aβ over this period. There was no change in cognitive index (mean [95% CI] 0.040 [-0.018, 0.098], p = 0.175) from before to 6 weeks after surgery, although there were postoperative declines in verbal memory (-0.346 [-0.523, -0.170], p = 0.003) and improvements in executive function (0.394, [0.310, 0.479], p < 0.001). There were no significant correlations between preoperative to 6-week postoperative changes in cognition and CSF tau, p-tau-181p, or Aβ42 changes over this interval (p > 0.05 for each).
Interpretation: Neurocognitive changes after non-cardiac, non-neurologic surgery in the majority of cognitively healthy, community-dwelling older adults are unlikely to be related to postoperative changes in AD neuropathology (as assessed by CSF Aβ, tau or p-tau-181p levels or the p-tau-181p/Aβ or tau/Aβ ratios).
Trial registration: clinicaltrials.gov (NCT01993836).
© 2022 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
M. B. has received material support (i.e., EEG monitor loan) for a postoperative recovery study in older adults from Masimo, and legal consulting fees related to postoperative neurocognitive function in older adults. J. N. B. acknowledges funding from Claret Medical, Inc. D. T. L. is an officer of AegisCN, which is developing the ApoE mimetic peptide CN‐105 for clinical use. The other authors have no other conflicts of interest to disclose related to this manuscript.
Figures
References
-
- 2021 Alzheimer's disease facts and figures. Alzheimers Dement. 2021;17(3):327‐406. - PubMed
-
- Chen CW, Lin CC, Chen KB, Kuo YC, Li CY, Chung CJ. Increased risk of dementia in people with previous exposure to general anesthesia: a nationwide population‐based case‐control study. Alzheimers Dement. 2014;10(2):196‐204. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- R03 AG050918/GF/NIH HHS/United States
- K76 AG057022/AG/NIA NIH HHS/United States
- R01 HL130443/HL/NHLBI NIH HHS/United States
- R03 AG050918/AG/NIA NIH HHS/United States
- U01-HL088942/GF/NIH HHS/United States
- U01 HL088942/HL/NHLBI NIH HHS/United States
- R01-AG042599/GF/NIH HHS/United States
- UL1TR002553-02/GF/NIH HHS/United States
- R01-HL130443/GF/NIH HHS/United States
- R01 AG042599/AG/NIA NIH HHS/United States
- K76-AG057022/GF/NIH HHS/United States
- UH2 AG056925-02/GF/NIH HHS/United States
- UL1 TR002553/TR/NCATS NIH HHS/United States
- P30 AG028716/AG/NIA NIH HHS/United States
- UH2 AG056925/AG/NIA NIH HHS/United States
- T32 GM008600/GM/NIGMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical