

The role of organizational characteristics on the outcome of COVID-19 patients admitted to the ICU in Belgium
- PMID: 35104305
- PMCID: PMC7757349
- DOI: 10.1016/j.lanepe.2020.100019
The role of organizational characteristics on the outcome of COVID-19 patients admitted to the ICU in Belgium
Abstract
Background: Several studies have investigated the predictors of in-hospital mortality for COVID-19 patients who need to be admitted to the Intensive Care Unit (ICU). However, no data on the role of organizational issues on patients' outcome are available in this setting. The aim of this study was therefore to assess the role of surge capacity organisation on the outcome of critically ill COVID-19 patients admitted to ICUs in Belgium.
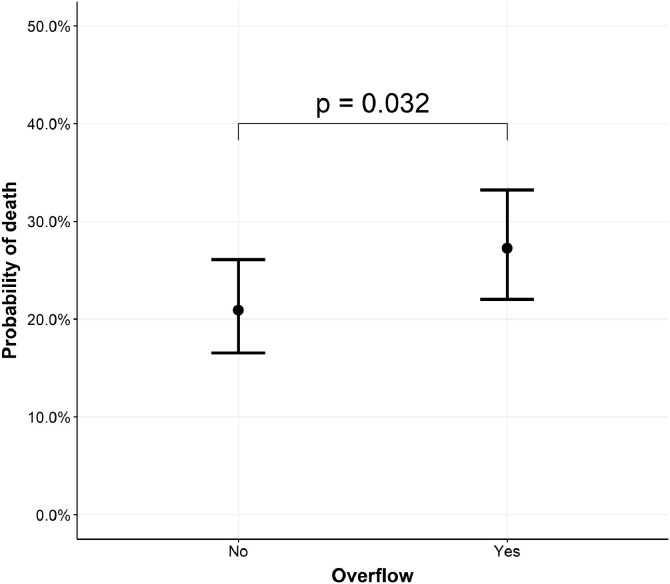
Methods: We conducted a retrospective analysis of in-hospital mortality in Belgian ICU COVID-19 patients via the national surveillance database. Non-survivors at hospital discharge were compared to survivors using multivariable mixed effects logistic regression analysis. Specific analyses including only patients with invasive ventilation were performed. To assess surge capacity, data were merged with administrative information on the type of hospital, the baseline number of recognized ICU beds, the number of supplementary beds specifically created for COVID-19 ICU care and the "ICU overflow" (i.e. a time-varying ratio between the number of occupied ICU beds by confirmed and suspected COVID-19 patients divided by the number of recognized ICU beds reserved for COVID-19 patients; ICU overflow was present when this ratio is ≥ 1.0).
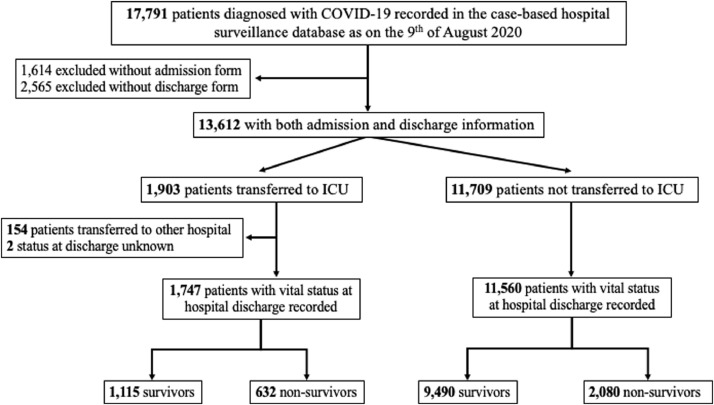
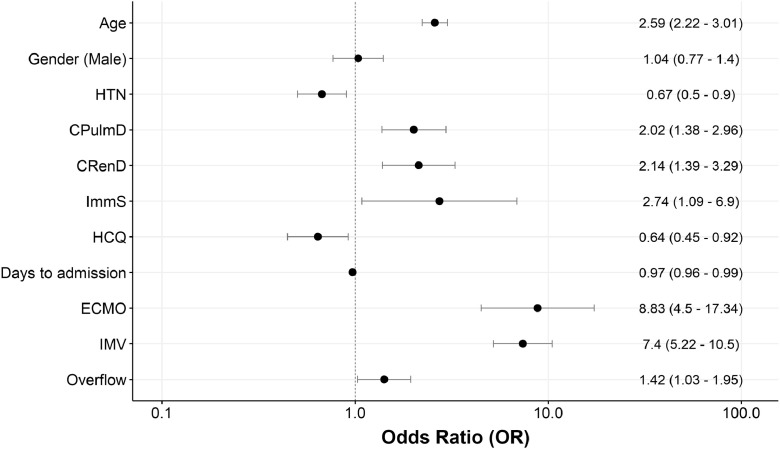
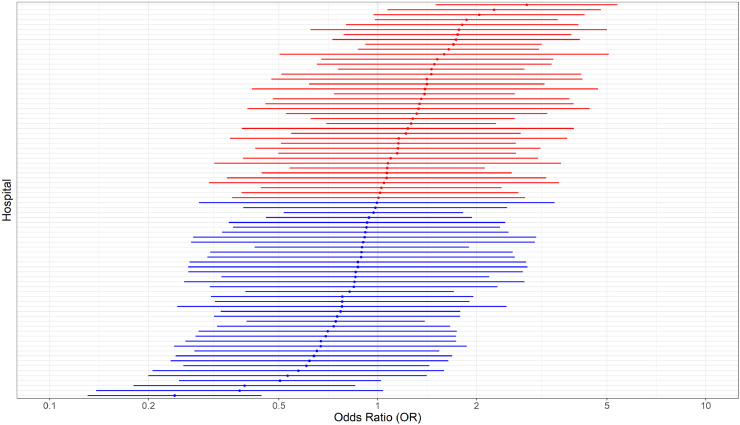
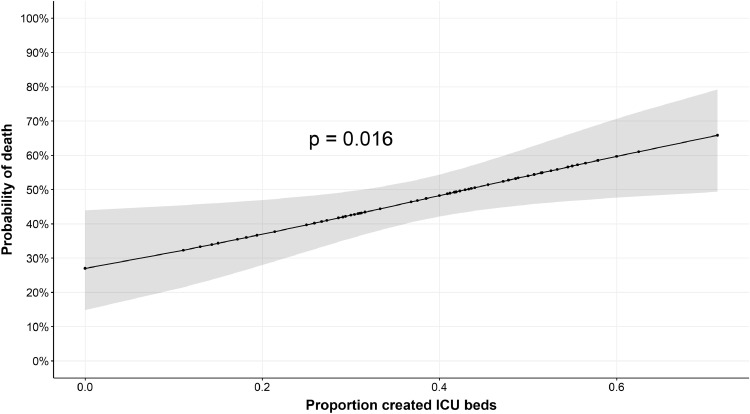
Findings: Over a total of 13,612 hospitalised COVID-19 patients with admission and discharge forms registered in the surveillance period (March, 1 to August, 9 2020), 1903 (14.0%) required ICU admission, of whom 1747 had available outcome data. Non-survivors (n = 632, 36.1%) were older and had more frequently various comorbid diseases than survivors. In the multivariable analysis, ICU overflow, together with older age, presence of comorbidities, shorter delay between symptom onset and hospital admission, absence of hydroxychloroquine therapy and use of invasive mechanical ventilation and of ECMO, was independently associated with an increased in-hospital mortality. Similar results were found in in in the subgroup of invasively ventilated patients. In addition, the proportion of supplementary beds specifically created for COVID-19 ICU care to the previously existing total number of ICU beds was associated with increased in-hospital mortality among invasively ventilated patients. The model also indicated a significant between-hospital difference in in-hospital mortality, not explained by the available patients and hospital characteristics.
Interpretation: Surge capacity organisation as reflected by ICU overflow or the creation of COVID-19 specific supplementary ICU beds were found to negatively impact ICU patient outcomes.
Funding: No funding source was available for this study.
Keywords: COVID-19; Intensive care unit; Mortality; Organisation; Surge.
© 2020 The Author(s).
Conflict of interest statement
FST received lecture fees from BD, Zoll, Nihon Khoden and Neuroptics, which are all outside the content of the present study. Other authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
