

Mucus Plugs Persist in Asthma, and Changes in Mucus Plugs Associate with Changes in Airflow over Time
- PMID: 35104436
- PMCID: PMC9851493
- DOI: 10.1164/rccm.202110-2265OC
Mucus Plugs Persist in Asthma, and Changes in Mucus Plugs Associate with Changes in Airflow over Time
Abstract
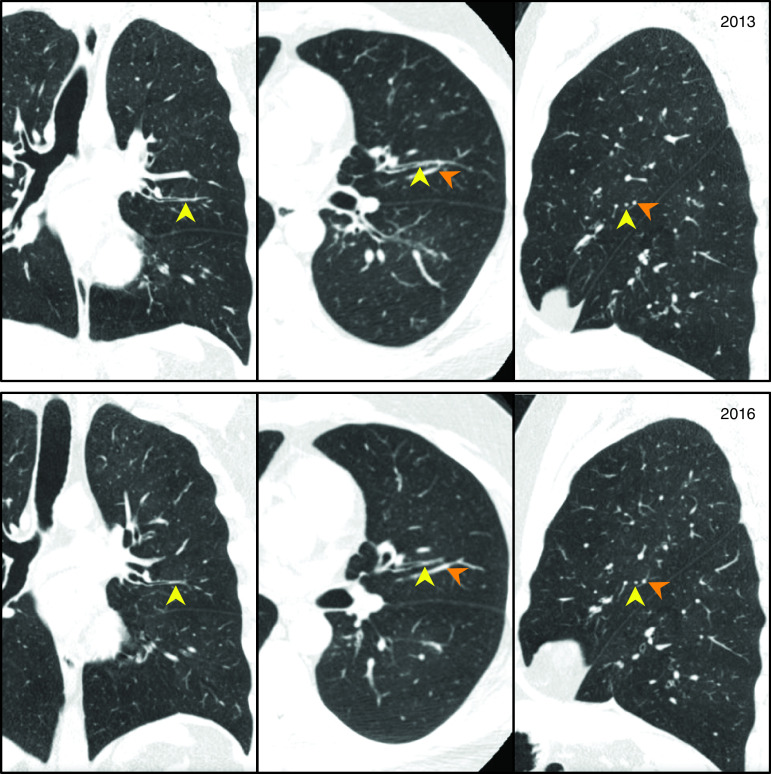
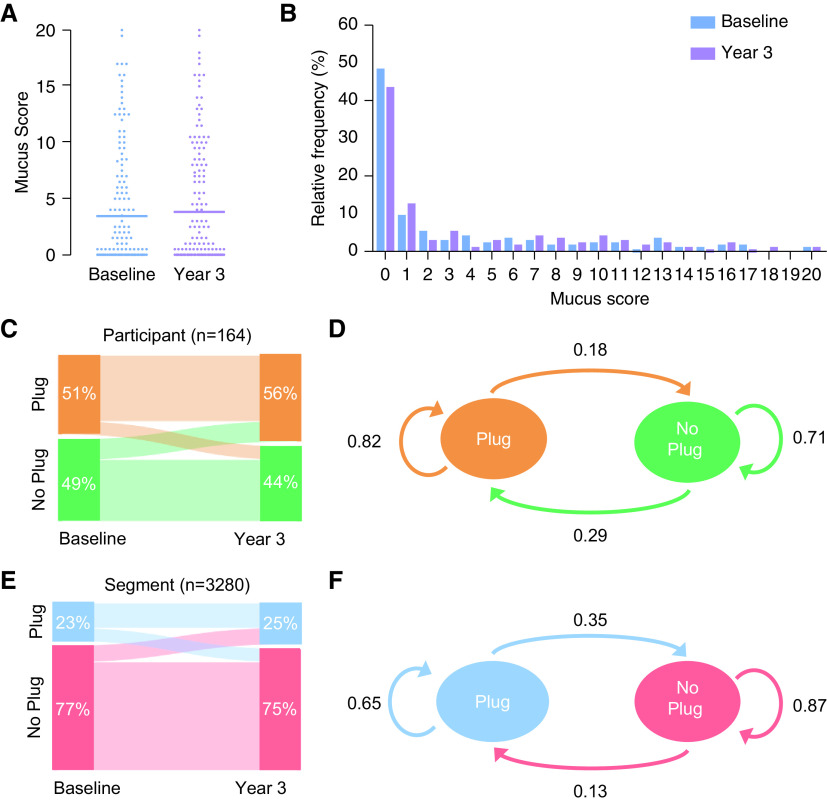
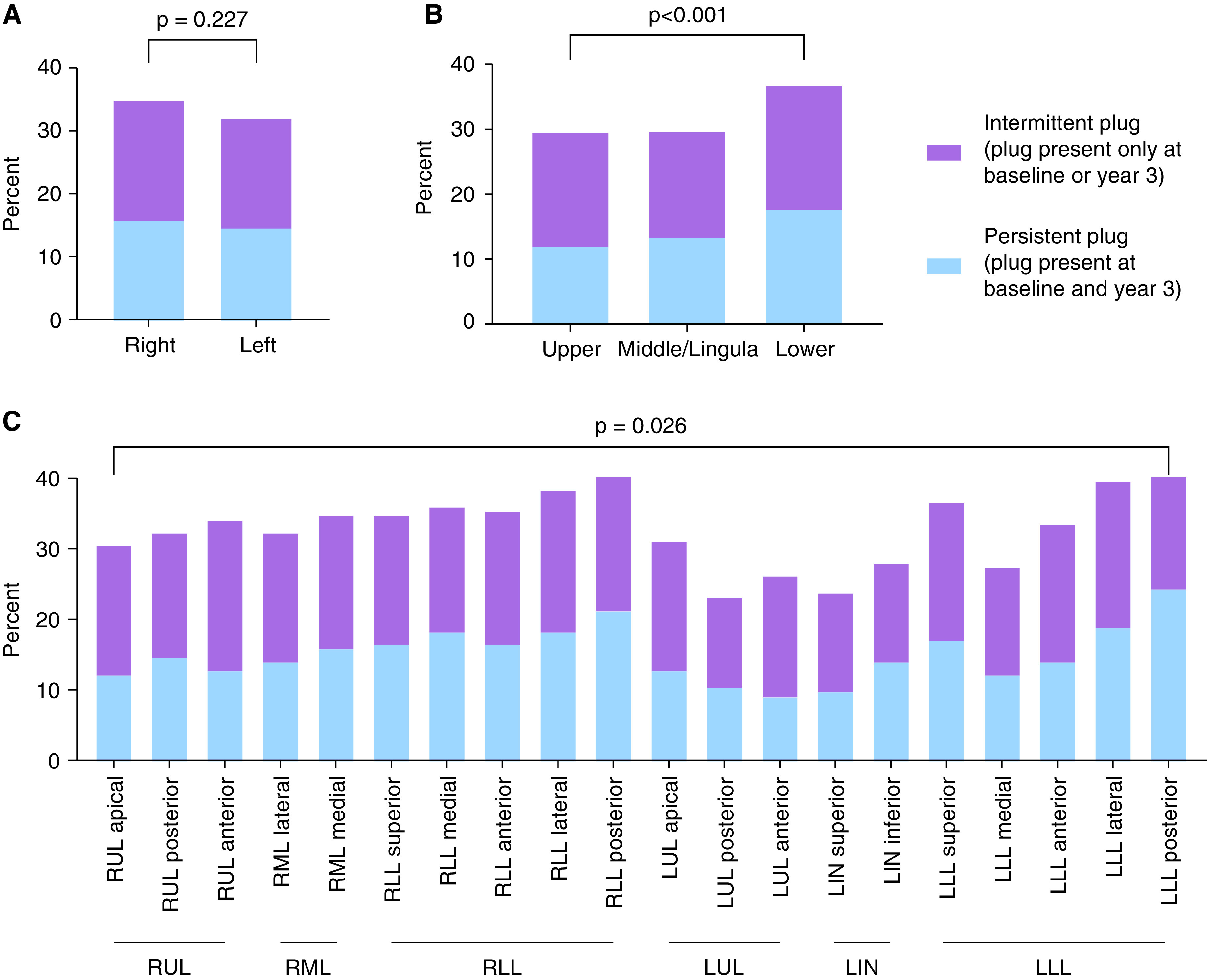
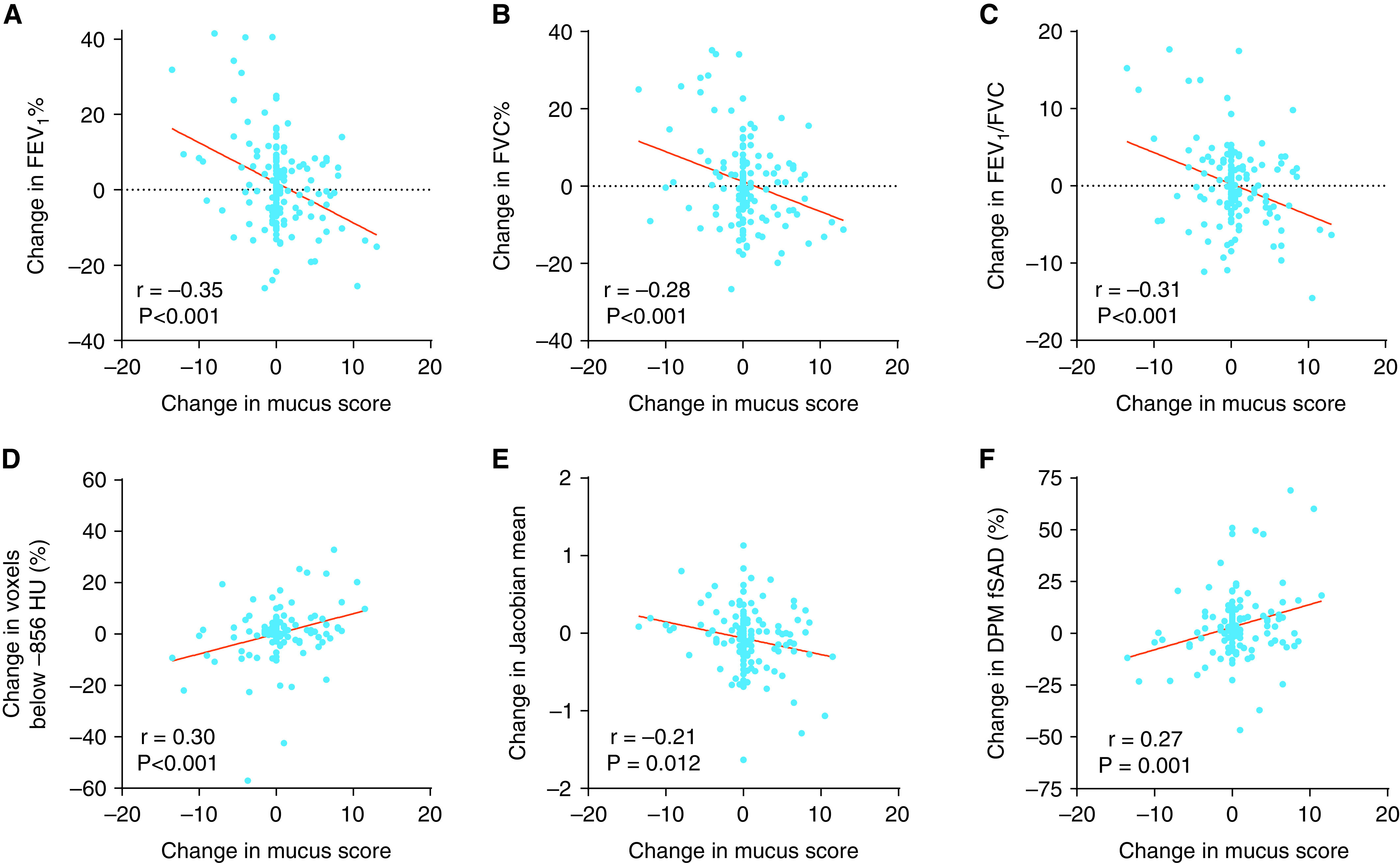
Rationale: Cross-sectional analysis of mucus plugs in computed tomography (CT) lung scans in the Severe Asthma Research Program (SARP)-3 showed a high mucus plug phenotype. Objectives: To determine if mucus plugs are a persistent asthma phenotype and if changes in mucus plugs over time associate with changes in lung function. Methods: In a longitudinal analysis of baseline and Year 3 CT lung scans in SARP-3 participants, radiologists generated mucus plug scores to assess mucus plug persistence over time. Changes in mucus plug score were analyzed in relation to changes in lung function and CT air trapping measures. Measurements and Main Results: In 164 participants, the mean (range) mucus plug score was similar at baseline and Year 3 (3.4 [0-20] vs. 3.8 [0-20]). Participants and bronchopulmonary segments with a baseline plug were more likely to have plugs at Year 3 than those without baseline plugs (risk ratio, 2.8; 95% confidence interval [CI], 2.0-4.1; P < 0.001; and risk ratio, 5.0; 95% CI, 4.5-5.6; P < 0.001, respectively). The change in mucus plug score from baseline to Year 3 was significantly negatively correlated with change in FEV1% predicted (rp = -0.35; P < 0.001) and with changes in CT air trapping measures (all P values < 0.05). Conclusions: Mucus plugs identify a persistent asthma phenotype, and susceptibility to mucus plugs occurs at the subject and the bronchopulmonary segment level. The association between change in mucus plug score and change in airflow over time supports a causal role for mucus plugs in mechanisms of airflow obstruction in asthma.
Keywords: air trapping; asthma; computed tomography; eosinophils; mucus plugs.
Figures
Comment in
-
Persistent Airway Plugs: A Call for Clinical Recognition and Novel Therapies.Am J Respir Crit Care Med. 2022 May 1;205(9):977-978. doi: 10.1164/rccm.202201-0147ED. Am J Respir Crit Care Med. 2022. PMID: 35259080 Free PMC article. No abstract available.
-
Statistical Concern Regarding the Relationship of Change in Mucus Plug Score with Airflow Over Time.Am J Respir Crit Care Med. 2022 Nov 15;206(10):1299. doi: 10.1164/rccm.202207-1273LE. Am J Respir Crit Care Med. 2022. PMID: 35876144 Free PMC article. No abstract available.
References
-
- Huber HL, Koessler KK. The pathology of bronchial asthma. Arch Intern Med . 1922;30:689–760.
-
- Cardell BS, Pearson RSB. Death in asthmatics. Thorax . 1959;14:341–352.
-
- Reid LM. The presence or absence of bronchial mucus in fatal asthma. J Allergy Clin Immunol . 1987;80:415–416. - PubMed
-
- Lang DM, Simon RA, Mathison DA, Timms RM, Stevenson DD. Safety and possible efficacy of fiberoptic bronchoscopy with lavage in the management of refractory asthma with mucous impaction. Ann Allergy . 1991;67:324–330. - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HL109257/HL/NHLBI NIH HHS/United States
- P30 ES005605/ES/NIEHS NIH HHS/United States
- P01 HL107202/HL/NHLBI NIH HHS/United States
- U01 HL146002/HL/NHLBI NIH HHS/United States
- K24 HL137013/HL/NHLBI NIH HHS/United States
- F32 HL162422/HL/NHLBI NIH HHS/United States
- U10 HL109250/HL/NHLBI NIH HHS/United States
- U19 AI077439/AI/NIAID NIH HHS/United States
- U10 HL109164/HL/NHLBI NIH HHS/United States
- U10 HL109086/HL/NHLBI NIH HHS/United States
- R01 HL080414/HL/NHLBI NIH HHS/United States
- U10 HL109172/HL/NHLBI NIH HHS/United States
- S10 OD025214/OD/NIH HHS/United States
- U10 HL109168/HL/NHLBI NIH HHS/United States
- U10 HL109152/HL/NHLBI NIH HHS/United States
- U10 HL109146/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
