

An Update on Laboratory Diagnostics in Haemophilia A and B
- PMID: 35104901
- PMCID: PMC9388220
- DOI: 10.1055/a-1665-6232
An Update on Laboratory Diagnostics in Haemophilia A and B
Abstract
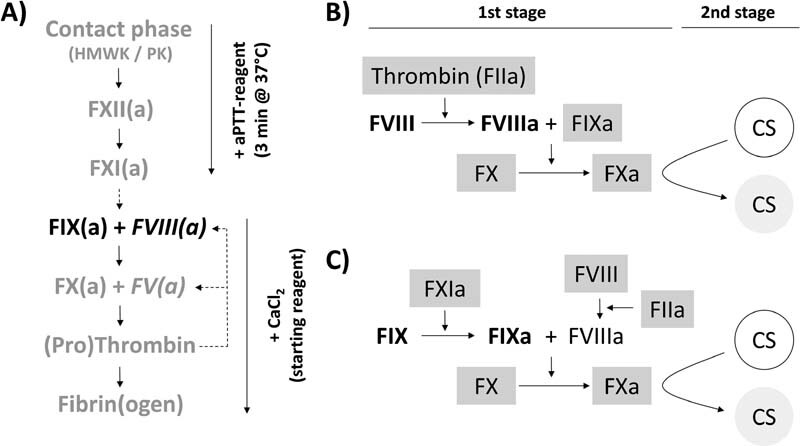
Haemophilia A (HA) and B (HB) are X-linked hereditary bleeding disorders caused by lack of activity of coagulation factors VIII (FVIII) or IX (FIX), respectively. Besides conventional products, modern replacement therapies include FVIII or FIX concentrates with an extended half-life (EHL-FVIII/FIX). Two main strategies for measuring plasma FVIII or FIX activity are applied: the one-stage clotting assay (OSCA) and the chromogenic substrate assay (CSA), both calibrated against plasma (FVIII/FIX) standards. Due to the structural modifications of EHL-FVIII/FIX, reagent-dependent assay discrepancies have been described when measuring the activity of these molecules. Assay discrepancies have also been observed in FVIII/FIX gene therapy approaches. On the other hand, nonfactor replacement by the bispecific antibody emicizumab, a FVIIIa-mimicking molecule, artificially shortens activated partial thromboplastin time-based clotting times, making standard OSCAs inapplicable for analysis of samples from patients treated with this drug. In this review, we aim to give an overview on both, the currently applied and future therapies in HA and HB with or without inhibitors and corresponding test systems suitable for accompanying diagnostics.
Bei der Hämophilie A (HA) und B (HB) handelt es sich um X-chromosomal vererbte Blutungsstörungen, die durch einen Mangel an Aktivität der Gerinnungsfaktoren VIII (FVIII) bzw. IX (FIX) verursacht werden. Im Rahmen entsprechender Substitutionstherapien kommen heute auch FVIII- oder FIX-Konzentrate mit einer verlängerten Halbwertszeit (EHL-FVIII/FIX) zum Einsatz. Zur Bestimmung der Aktivität von FVIII- bzw. FIX werden zwei grundlegend verschiedene Testprinzipien angewandt, Einstufen-Gerinnungstests (One-Stage Clotting Assay [OSCA]) und chromogene Testverfahren (CS-Assays [CSA]), welche gegen plasmatische Faktoren kalibriert werden. Aufgrund der strukturellen Modifikationen von EHL-FVIII/FIX sind testabhängige Diskrepanzen bei der Bestimmung der Aktivität dieser Moleküle beschrieben worden. Solche Diskrepanzen wurden auch im Rahmen der FVIII-/FIX-Gentherapie beobachtet. Unter Emicizumab, einem bispezifischen, monoklonalen Antikörper zur Behandlung der HA, sind die Gerinnungszeiten der aktivierten partiellen Thromboplastinzeit (aPTT) artifiziell verkürzt. Dadurch sind etablierte, aPTT-basierte Einstufen-Gerinnungstests für die Analyze von Proben von Patienten unter Emicizumab nicht anwendbar. Mit dieser Übersichtsarbeit soll ein Überblick sowohl über die Prinzipien der derzeit angewandten und zukünftigen Therapieoptionen als auch über entsprechende Testverfahren in der HA und HB gegeben werden.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Bolton-Maggs P H, Pasi K J.Haemophilias A and B Lancet 2003361(9371)1801–1809. - PubMed
-
- Chowdary P. Extended half-life recombinant products in haemophilia clinical practice - expectations, opportunities and challenges. Thromb Res. 2020;196:609–617. - PubMed
-
- Cormier M, Batty P, Tarrant J, Lillicrap D. Advances in knowledge of inhibitor formation in severe haemophilia A. Br J Haematol. 2020;189(01):39–53. - PubMed
-
- Burness C B, Scott L J. Susoctocog alfa: a review in acquired haemophilia A. Drugs. 2016;76(07):815–821. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical