

Trends in percentages of gestational diabetes mellitus attributable to overweight, obesity, and morbid obesity in regional Victoria: an eight-year population-based panel study
- PMID: 35105311
- PMCID: PMC8809044
- DOI: 10.1186/s12884-022-04420-9
Trends in percentages of gestational diabetes mellitus attributable to overweight, obesity, and morbid obesity in regional Victoria: an eight-year population-based panel study
Abstract
Background: Gestational diabetes mellitus (GDM) is the fastest growing type of diabetes in Australia with rates trebling over the past decades partially explained by rising obesity rates and maternal age among childbearing women. Percentage of GDM attributable to obesity has been documented, mostly focusing on metropolitan populations. In parts of regional (areas outside capital cities) and rural Australia where overweight, obesity and morbid obesity are more prevalent, intertwined with socioeconomic disadvantage and higher migrant communities, trends over time in adjusted percentages of GDM attributed to obesity are unknown.
Methods: In this population-based retrospective panel study, women, without pre-existing diabetes, delivering singletons between 2010 and 2017 in a tertiary regional hospital that serves 26% of Victoria's 6.5 million Australian population were eligible for inclusion. Secular trends in GDM by body mass index (BMI) and age were evaluated. The percentage of GDM that would have been prevented each year with the elimination of overweight or obesity was estimated using risk-adjusted regression-based population attributable fractions (AFp). Trends in the AFp over time were tested using the augmented Dickey-Fuller test.
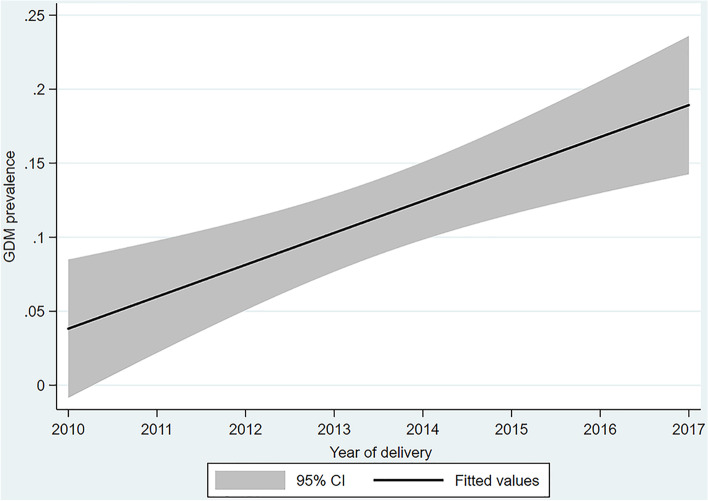
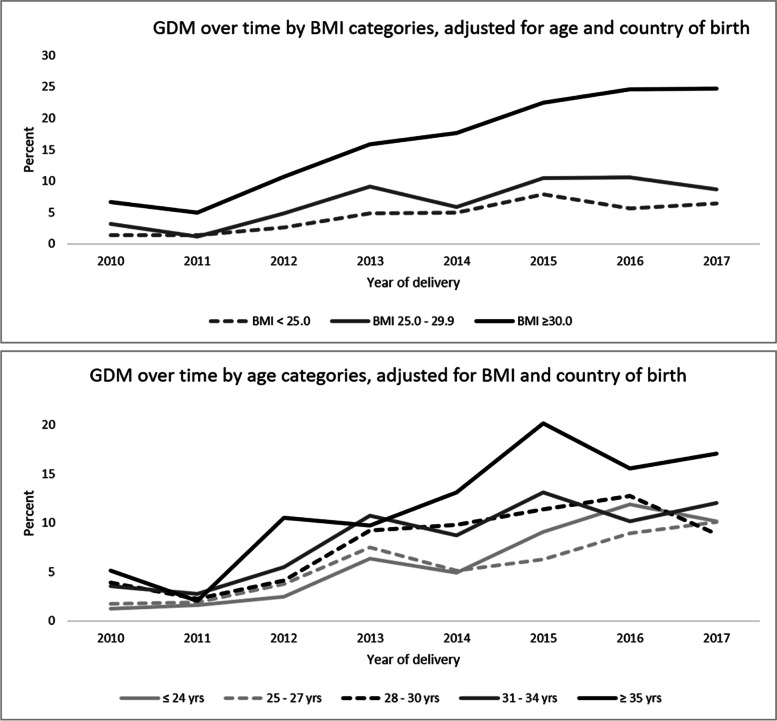
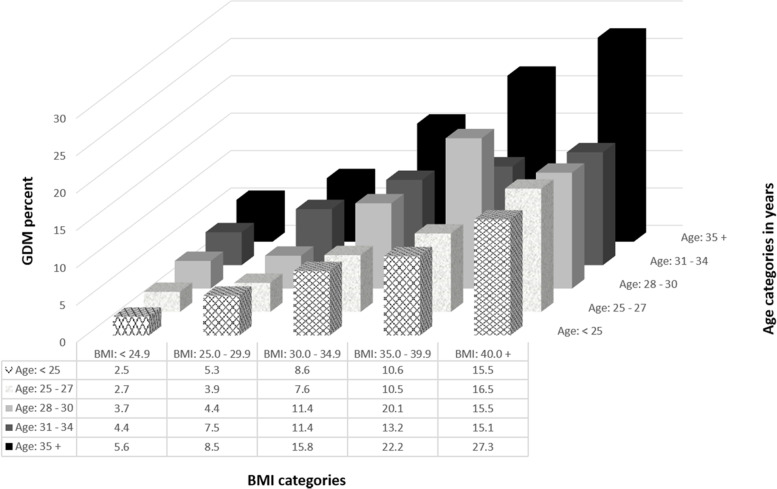
Results: Overall 7348 women, contributing to 10,028 births were included. The age of expecting mothers, their BMI, proportion of women born overseas, and GDM incidence significantly rose over time with GDM rising from 3.5% in 2010 to 13.7% in 2017, p < 0.001, increasing in all BMI categories. The incidence was consistently highest among women with obesity (13.8%) and morbid obesity (21.6%). However, the highest relative increase was among women with BMI < 25 kg/m2, rising from 1.4% in 2010 to 7.0% in 2017. Adjusting for age, country of birth, socioeconomic status, comorbidities, antenatal and intrapartum factors, an estimated 8.6% (confidence interval (CI) 6.1-11.0%), 15.6% (95% CI 12.2-19.0%), and 19.5% (95% CI 15.3-23.6%) of GDM would have been prevented by eliminating maternal overweight, obesity, and morbid obesity, respectively. However, despite the rise in obesity over time, percentages of GDM attributable to overweight, obesity, and morbid obesity significantly dropped over time. Scenario analyses supported these findings.
Conclusions: Besides increasing prevalence of obesity over time, this study suggests that GDM risk factors, other than obesity, are also increasing over time.
Keywords: Gestational diabetes mellitus; Incidence; Obesity; Population attributable fractions; Trends.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Aguirre F, Brown A, Cho NH, Dahlquist G, Dodd S, Dunning T, et al. IDF Diabetes Atlas: Sixth edition. Sixth ed. International Diabetes Federation. 2013. p. 160.
-
- Hod M, Kapur A, Sacks DA, Hadar E, Agarwal M, Di Renzo GC, et al. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on gestational diabetes mellitus: A pragmatic guide for diagnosis, management, and care. Int J Gynaecol Obstet. 2015;131(Suppl 3):S173–S211. - PubMed
-
- Chen Y, Quick WW, Yang W, Zhang Y, Baldwin A, Moran J, et al. Cost of gestational diabetes mellitus in the United States in 2007. Popul Health Manag. 2009;12:165–174. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
