

EPHA2 mediates PDGFA activity and functions together with PDGFRA as prognostic marker and therapeutic target in glioblastoma
- PMID: 35105853
- PMCID: PMC8807725
- DOI: 10.1038/s41392-021-00855-2
EPHA2 mediates PDGFA activity and functions together with PDGFRA as prognostic marker and therapeutic target in glioblastoma
Abstract
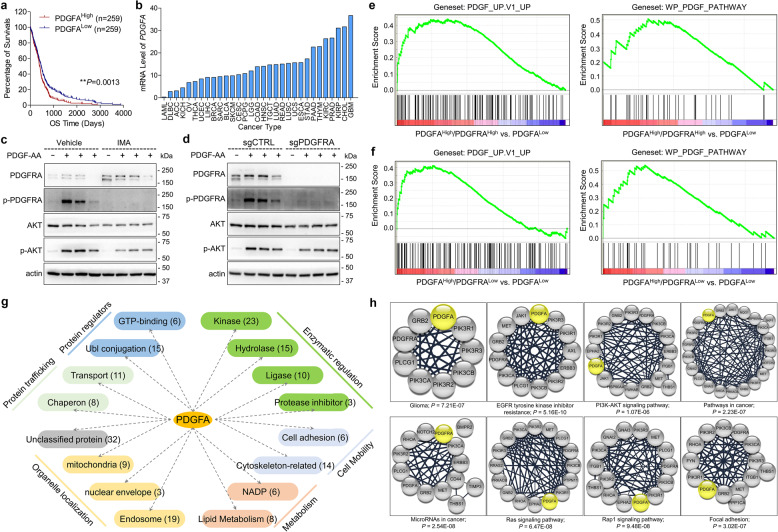
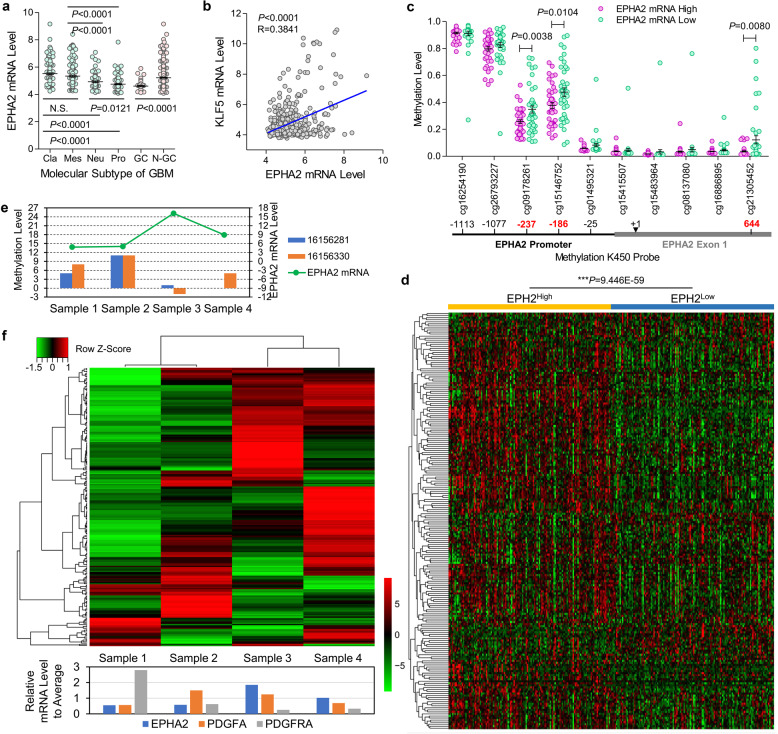
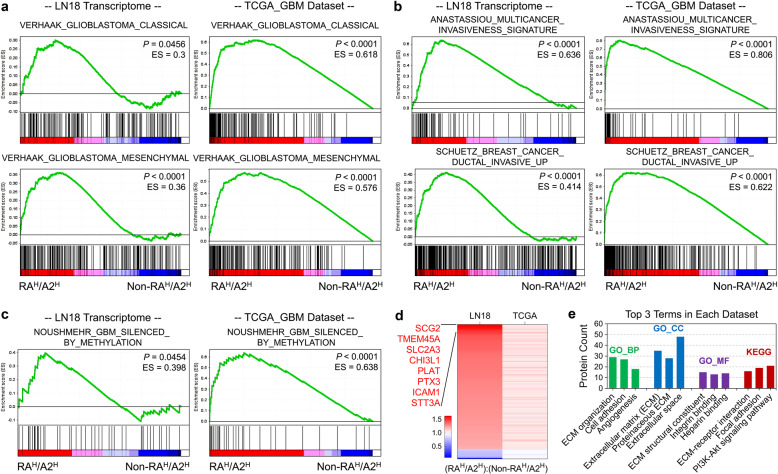
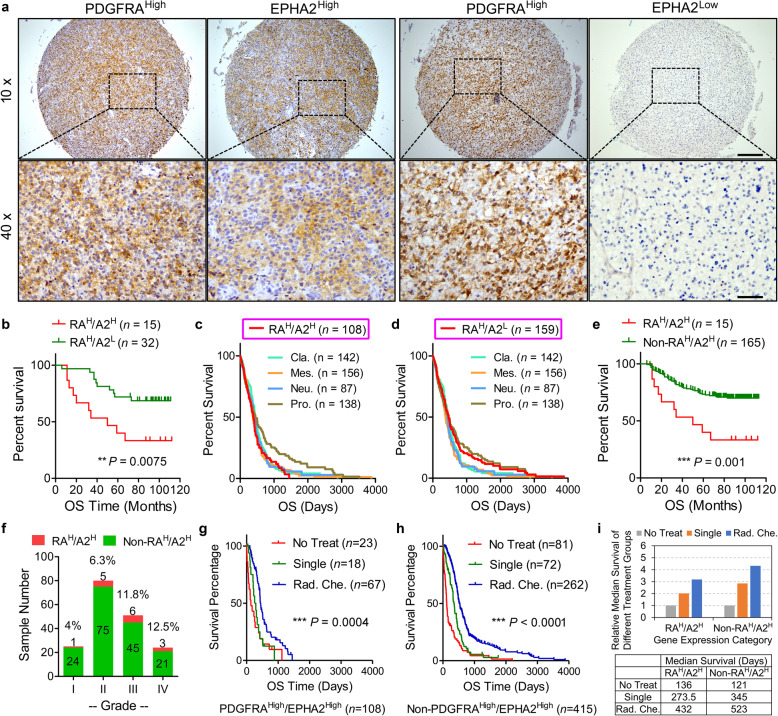
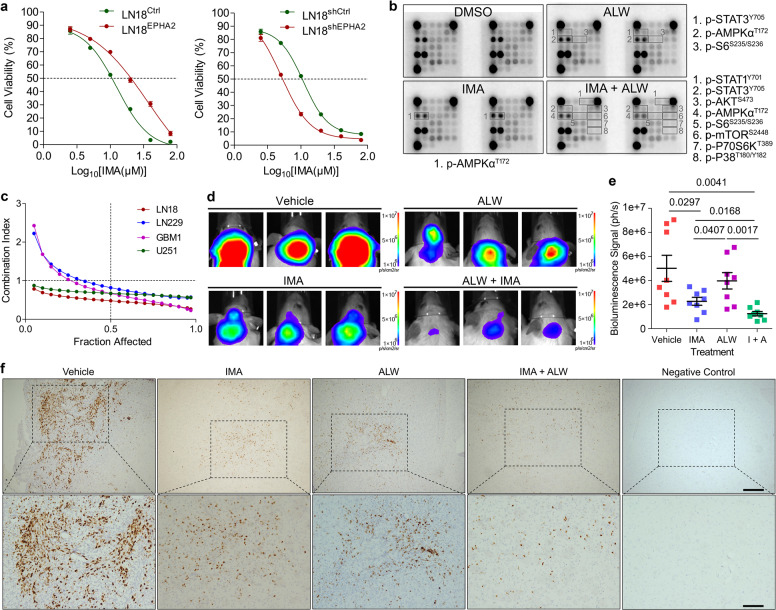
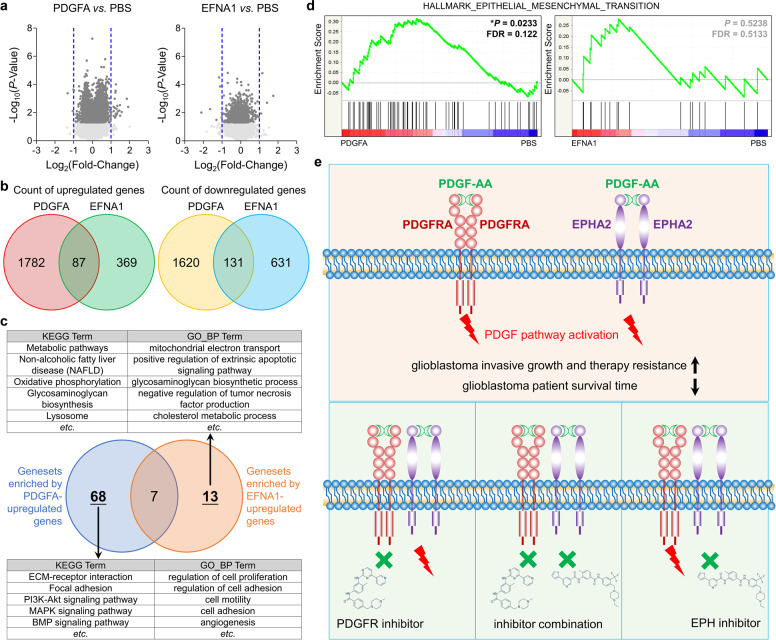
Platelet-derived growth subunit A (PDGFA) plays critical roles in development of glioblastoma (GBM) with substantial evidence from TCGA database analyses and in vivo mouse models. So far, only platelet-derived growth receptor α (PDGFRA) has been identified as receptor for PDGFA. However, PDGFA and PDGFRA are categorized into different molecular subtypes of GBM in TCGA_GBM database. Our data herein further showed that activity or expression deficiency of PDGFRA did not effectively block PDGFA activity. Therefore, PDGFRA might be not necessary for PDGFA function.To profile proteins involved in PDGFA function, we performed co-immunoprecipitation (Co-IP) and Mass Spectrum (MS) and delineated the network of PDGFA-associated proteins for the first time. Unexpectedly, the data showed that EPHA2 could be temporally activated by PDGFA even without activation of PDGFRA and AKT. Furthermore, MS, Co-IP, in vitro binding thermodynamics, and proximity ligation assay consistently proved the interaction of EPHA2 and PDGFA. In addition, we observed that high expression of EPHA2 leaded to upregulation of PDGF signaling targets in TCGA_GBM database and clinical GBM samples. Co-upregulation of PDGFRA and EPHA2 leaded to worse patient prognosis and poorer therapeutic effects than other contexts, which might arise from expression elevation of genes related with malignant molecular subtypes and invasive growth. Due to PDGFA-induced EPHA2 activation, blocking PDGFRA by inhibitor could not effectively suppress proliferation of GBM cells, but simultaneous inhibition of both EPHA2 and PDGFRA showed synergetic inhibitory effects on GBM cells in vitro and in vivo. Taken together, our study provided new insights on PDGFA function and revealed EPHA2 as a potential receptor of PDGFA. EPHA2 might contribute to PDGFA signaling transduction in combination with PDGFRA and mediate the resistance of GBM cells to PDGFRA inhibitor. Therefore, combination of inhibitors targeting PDGFRA and EHA2 represented a promising therapeutic strategy for GBM treatment.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests. X.-W.B. is the editorial board member of Signal Transduction and Targeted Therapy, but he has not been involved in the process of the manuscript handling.
Figures

References
-
- Louis DN, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol. 2016;131:803–820. - PubMed
-
- Ohgaki H, Kleihues P. Population-based studies on incidence, survival rates, and genetic alterations in astrocytic and oligodendroglial gliomas. J. Neuropathol. Exp. Neurol. 2005;64:479–489. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
