

Effect of implantable cardioverter-defibrillators in patients with non-ischaemic systolic heart failure and concurrent coronary atherosclerosis
- PMID: 35106935
- PMCID: PMC8934968
- DOI: 10.1002/ehf2.13810
Effect of implantable cardioverter-defibrillators in patients with non-ischaemic systolic heart failure and concurrent coronary atherosclerosis
Abstract
Aims: Prophylactic implantable cardioverter-defibrillators (ICD) reduce mortality in patients with ischaemic heart failure (HF), whereas the effect of ICD in patients with non-ischaemic HF is less clear. We aimed to investigate the association between concomitant coronary atherosclerosis and mortality in patients with non-ischaemic HF and the effect of ICD implantation in these patients.
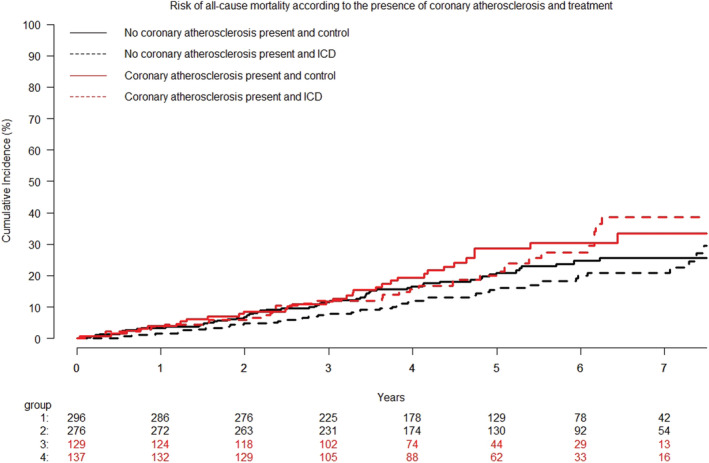
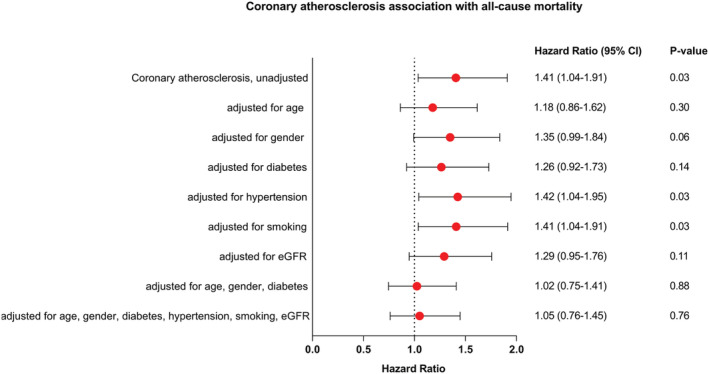
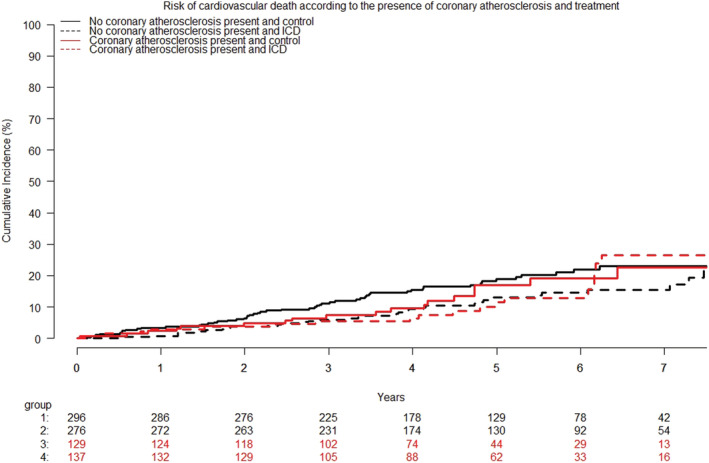
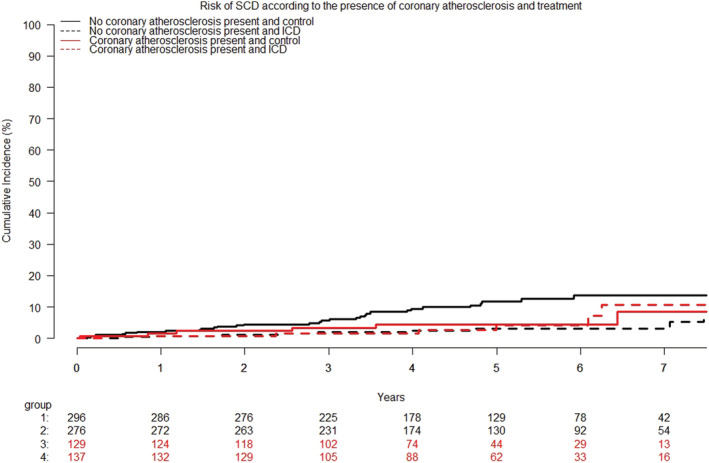
Methods and results: Patients were included from DANISH (Danish Study to Assess the Efficacy of Implantable Cardioverter Defibrillators in Patients with Non-Ischaemic Systolic Heart Failure on Mortality), randomizing patients to ICD or control. Study inclusion criteria for HF were left ventricular ejection fraction ≤ 35% and increased levels (>200 pg/mL) of N-terminal pro-brain natriuretic peptide. Of the 1116 patients from DANISH, 838 (75%) patients had available data from coronary angiogram and were included in this subgroup analysis. We used Cox regression to assess the relationship between coronary atherosclerosis and mortality and the effect of ICD implantation. Of the included patients, 266 (32%) had coronary atherosclerosis. Of these, 216 (81%) had atherosclerosis without significant stenoses, and 50 (19%) had significant stenosis. Patients with atherosclerosis were significantly older {67 [interquartile range (IQR) 61-73] vs. 61 [IQR 54-68] years; P < 0.0001}, and more were men (77% vs. 70%; P = 0.03). During a median follow-up of 64.3 months (IQR 47-82), 174 (21%) of the patients died. The effect of ICD on all-cause mortality was not modified by coronary atherosclerosis [hazard ratio (HR) 0.94; 0.58-1.52; P = 0.79 vs. HR 0.82; 0.56-1.20; P = 0.30], P for interaction = 0.67. In univariable analysis, coronary atherosclerosis was a significant predictor of all-cause mortality [HR, 1.41; 95% confidence interval (CI), 1.04-1.91; P = 0.03]. However, this association disappeared when adjusting for cardiovascular risk factors (age, gender, diabetes, hypertension, smoking, and estimated glomerular filtration rate) (HR 1.05, 0.76-1.45, P = 0.76).
Conclusions: In patients with non-ischaemic systolic heart failure, ICD implantation did not reduce all-cause mortality in patients either with or without concomitant coronary atherosclerosis. The concomitant presence of coronary atherosclerosis was associated with increased mortality. However, this association was explained by other risk factors.
Keywords: Coronary atherosclerosis; Implantable cardioverter defibrillator; Mortality; Non-ischaemic systolic heart failure.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
Christina Byrne, Ole Ahlehoff, Marie Bayer Elming, Frants Pedersen, Hans Eiskjær, Anna Margrethe Thøgersen, Jens Haarbo, Lars Videbæk, Lars Køber, and Jens Jakob Thune report no conflicts of interest related to the present manuscript. Jens Cosedis Nielsen is supported by a grant from the Novo Nordisk Foundation (NNF16OC0018658). Jesper Hastrup Svendsen has received research grants outside the present study and personal speaker fee from Medtronic. Steen Pehrson has received personal speaker fee from Abbott.
Figures
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González‐Juanatey JR, Harjola V‐P, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016; 37: 2129–2200. - PubMed
-
- Felker GM, Thompson RE, Hare JM, Hruban RH, Clemetson DE, Howard DL, Baughman KL, Kasper EK. Underlying causes and long‐term survival in patients with initially unexplained cardiomyopathy. N Engl J Med 2000; 342: 1077–1084. - PubMed
-
- Gheorghiade M, Sopko G, De Luca L, Velazquez EJ, Parker JD, Binkley PF, Sadowski Z, Golba KS, Prior DL, Rouleau JL, Bonow RO. Navigating the crossroads of coronary artery disease and heart failure. Circulation 2006; 114: 1202–1213. - PubMed
-
- Moss AJ, Hall WJ, Cannom DS, Daubert JP, Higgins SL, Klein H, Levine JH, Saksena S, Waldo AL, Wilber D, Brown MW, Heo M. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter automatic defibrillator implantation trial investigators. N Engl J Med 1996; 335: 1933–1940. - PubMed
-
- Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN, Hafley G. A randomized study of the prevention of sudden death in patients with coronary artery disease. Multicenter unsustained tachycardia trial investigators. N Engl J Med 1999; 341: 1882–1890. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
