

Randomized Clinical Study of Temporary Transvenous Phrenic Nerve Stimulation in Difficult-to-Wean Patients
- PMID: 35108175
- PMCID: PMC9872796
- DOI: 10.1164/rccm.202107-1709OC
Randomized Clinical Study of Temporary Transvenous Phrenic Nerve Stimulation in Difficult-to-Wean Patients
Abstract
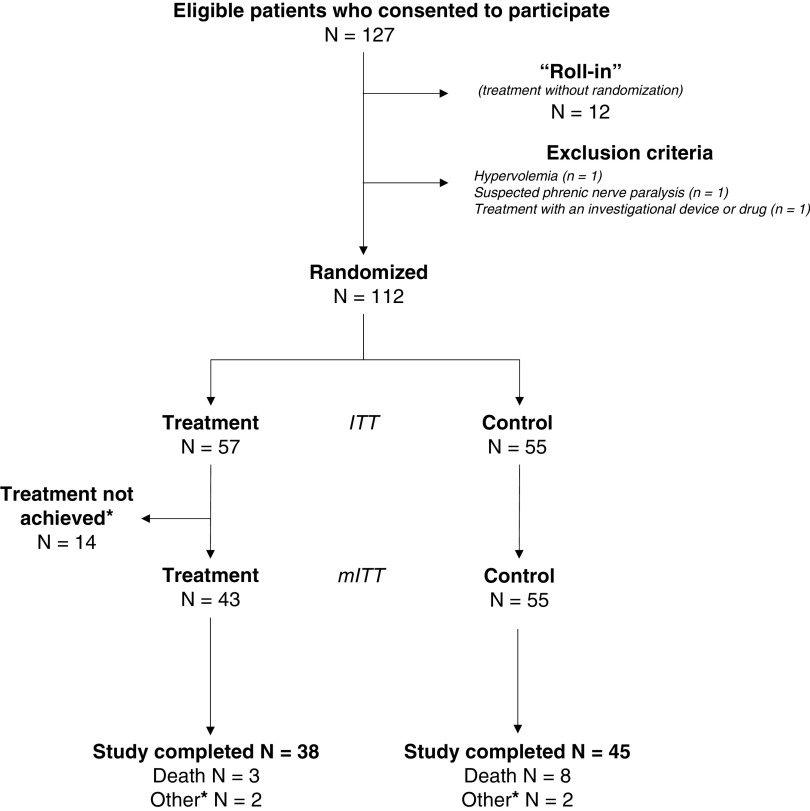
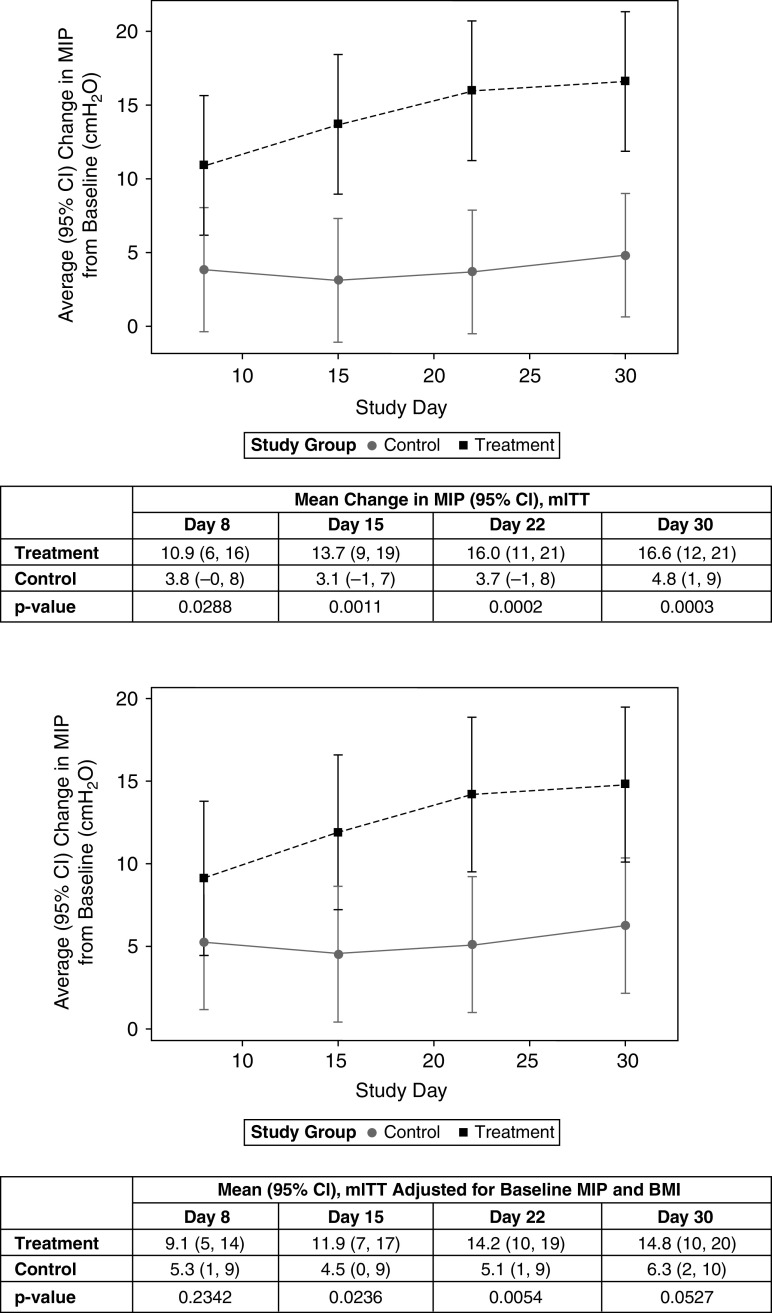
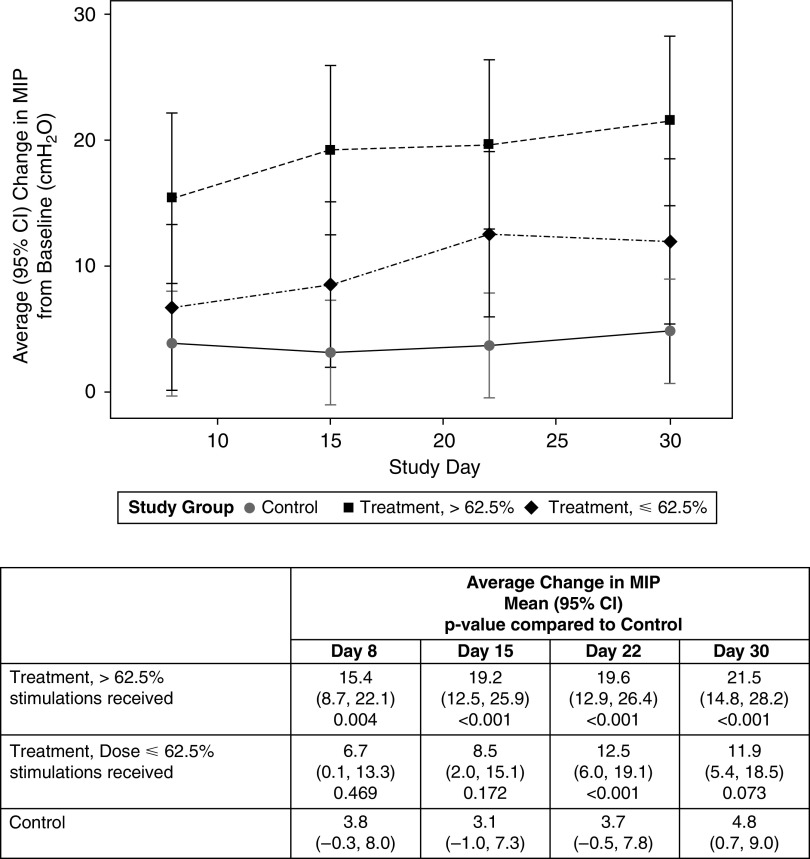
Rationale: Diaphragm dysfunction is frequently observed in critically ill patients with difficult weaning from mechanical ventilation. Objectives: To evaluate the effects of temporary transvenous diaphragm neurostimulation on weaning outcome and maximal inspiratory pressure. Methods: Multicenter, open-label, randomized, controlled study. Patients aged ⩾18 years on invasive mechanical ventilation for ⩾4 days and having failed at least two weaning attempts received temporary transvenous diaphragm neurostimulation using a multielectrode stimulating central venous catheter (bilateral phrenic stimulation) and standard of care (treatment) (n = 57) or standard of care (control) (n = 55). In seven patients, the catheter could not be inserted, and in seven others, pacing therapy could not be delivered; consequently, data were available for 43 patients. The primary outcome was the proportion of patients successfully weaned. Other endpoints were mechanical ventilation duration, 30-day survival, maximal inspiratory pressure, diaphragm-thickening fraction, adverse events, and stimulation-related pain. Measurements and Main Results: The incidences of successful weaning were 82% (treatment) and 74% (control) (absolute difference [95% confidence interval (CI)], 7% [-10 to 25]), P = 0.59. Mechanical ventilation duration (mean ± SD) was 12.7 ± 9.9 days and 14.1 ± 10.8 days, respectively, P = 0.50; maximal inspiratory pressure increased by 16.6 cm H2O and 4.8 cm H2O, respectively (difference [95% CI], 11.8 [5 to 19]), P = 0.001; and right hemidiaphragm thickening fraction during unassisted spontaneous breathing was +17% and -14%, respectively, P = 0.006, without correlation with changes in maximal inspiratory pressure. Serious adverse event frequency was similar in both groups. Median stimulation-related pain in the treatment group was 0 (no pain). Conclusions: Temporary transvenous diaphragm neurostimulation did not increase the proportion of successful weaning from mechanical ventilation. It was associated with a significant increase in maximal inspiratory pressure, suggesting reversal of the course of diaphragm dysfunction. Clinical trial registered with www.clinicaltrials.gov (NCT03096639) and the European Database on Medical Devices (CIV-17-06-020004).
Keywords: diaphragm weakness; mechanical ventilation; ventilator-induced diaphragmatic dysfunction; weaning.
Figures
Comment in
-
Transvenous Phrenic Nerve Stimulation: A Novel Therapy Gathering Pace.Am J Respir Crit Care Med. 2022 May 15;205(10):1135-1136. doi: 10.1164/rccm.202202-0315ED. Am J Respir Crit Care Med. 2022. PMID: 35320061 Free PMC article. No abstract available.
-
Transvenous Phrenic Nerve Stimulation in Patients Who Are Difficult to Wean.Am J Respir Crit Care Med. 2022 Oct 15;206(8):1047. doi: 10.1164/rccm.202206-1024LE. Am J Respir Crit Care Med. 2022. PMID: 35772121 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
