

Development of a nomogram for the prediction of in-hospital mortality in patients with acute ST-elevation myocardial infarction after primary percutaneous coronary intervention: a multicentre, retrospective, observational study in Hebei province, China
- PMID: 35110324
- PMCID: PMC8811571
- DOI: 10.1136/bmjopen-2021-056101
Development of a nomogram for the prediction of in-hospital mortality in patients with acute ST-elevation myocardial infarction after primary percutaneous coronary intervention: a multicentre, retrospective, observational study in Hebei province, China
Abstract
Objectives: To establish a clinical prognostic nomogram for predicting in-hospital mortality after primary percutaneous coronary intervention (PCI) among patients with ST-elevation myocardial infarction (STEMI).
Design: Retrospective, multicentre, observational study.
Setting: Thirty-nine hospitals in Hebei province.
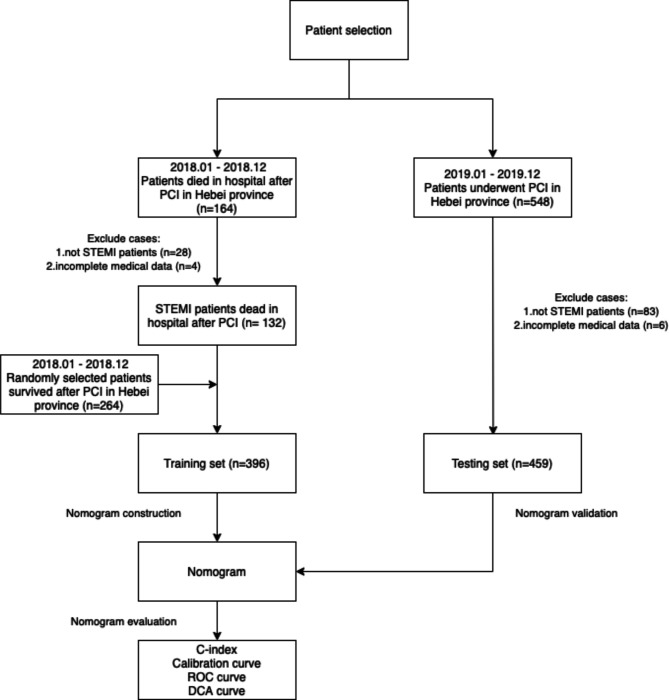
Participants: Patients with STEMI who underwent PCI from January 2018 to December 2019.
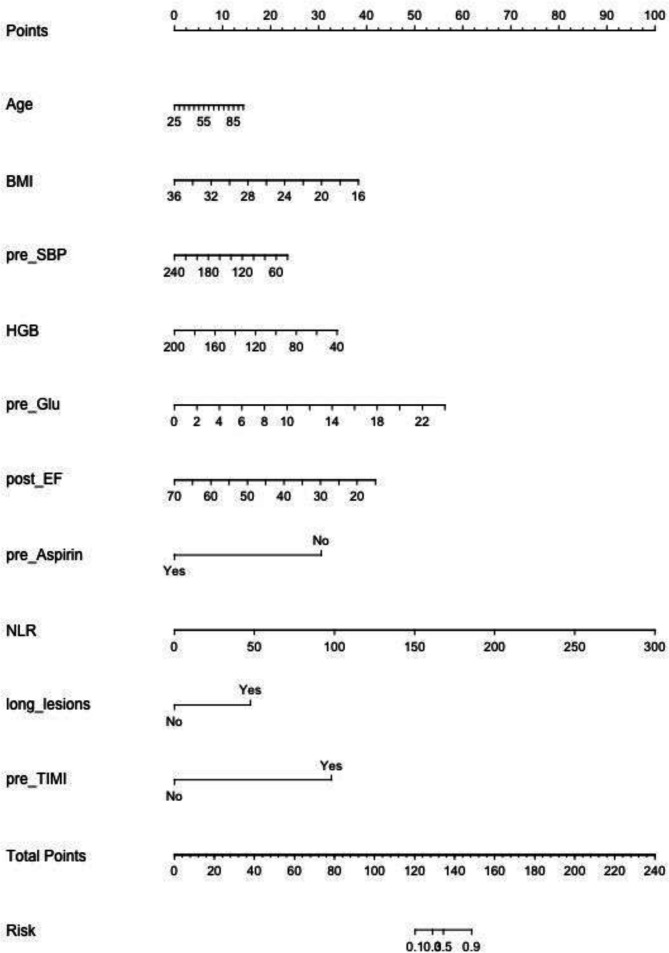
Interventions: A multivariable logistic regression model was used to identify the factors associated with in-hospital mortality, and a nomogram was established using these factors. The performance of the nomogram was evaluated by the discrimination, calibration and clinical usefulness.
Primary and secondary outcome measures: The outcome was the factors associated with in-hospital mortality.
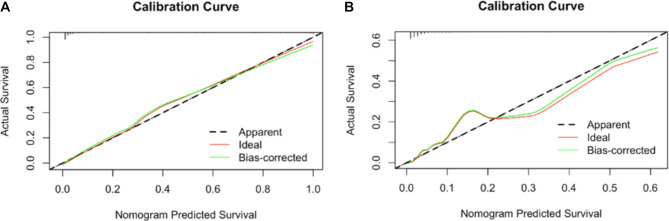
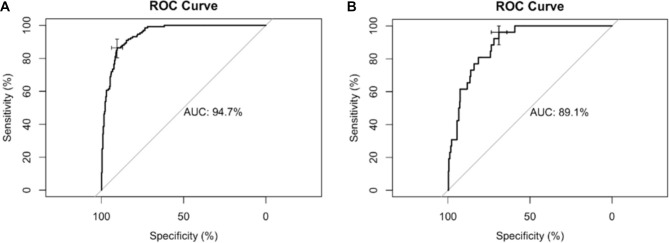
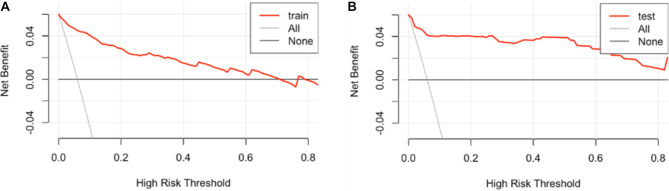
Results: This study included 855 patients, among whom 223 died in hospital. Age, body mass index, systolic pressure on admission, haemoglobin, random blood glucose on admission, ejection fraction after PCI, use aspirin before admission, long lesions, thrombolysis in myocardial infarction flow grade and neutrophils/lymphocytes ratio were independently associated with in-hospital mortality (all p<0.05). In the training set, the nomogram showed a C-index of 0.947, goodness-of-fit of 0.683 and area under the receiver operating characteristic curve (AUC) of 0.947 (95% CI 0.927 to 0.967). In the testing set, the C-index was 0.891, goodness-of-fit was 0.462 and AUC was 0.891 (95% CI 0.844 to 0.939). The results indicate that the nomogram had good discrimination and good prediction accuracy and could achieve a good net benefit.
Conclusions: A nomogram to predict in-hospital mortality in patients with STEMI after PCI was developed and validated in Hebei, China and showed a satisfactory performance. Prospective studies will be necessary to confirm the performance and clinical applicability and practicality of the nomogram.
Keywords: coronary heart disease; coronary intervention; myocardial infarction.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Nomogram for Predicting In-Hospital Mortality in Patients with Acute ST-Elevation Myocardial Infarction Complicated by Cardiogenic Shock after Primary Percutaneous Coronary Intervention.J Interv Cardiol. 2022 Mar 12;2022:8994106. doi: 10.1155/2022/8994106. eCollection 2022. J Interv Cardiol. 2022. PMID: 35356419 Free PMC article.
-
Establishment and validation of a risk model for prediction of in-hospital mortality in patients with acute ST-elevation myocardial infarction after primary PCI.BMC Cardiovasc Disord. 2020 Dec 9;20(1):513. doi: 10.1186/s12872-020-01804-7. BMC Cardiovasc Disord. 2020. PMID: 33297955 Free PMC article.
-
Construction and evaluation of nomogram model for individualized prediction of risk of major adverse cardiovascular events during hospitalization after percutaneous coronary intervention in patients with acute ST-segment elevation myocardial infarction.Front Cardiovasc Med. 2022 Dec 21;9:1050785. doi: 10.3389/fcvm.2022.1050785. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36620648 Free PMC article.
-
Predictive value of neutrophil to lymphocyte ratio in patients with acute ST segment elevation myocardial infarction after percutaneous coronary intervention: a meta-analysis.BMC Cardiovasc Disord. 2018 May 2;18(1):75. doi: 10.1186/s12872-018-0812-6. BMC Cardiovasc Disord. 2018. PMID: 29716535 Free PMC article. Review.
-
Mortality prediction algorithms for patients undergoing primary percutaneous coronary intervention.J Thorac Dis. 2020 Apr;12(4):1706-1720. doi: 10.21037/jtd.2019.12.83. J Thorac Dis. 2020. PMID: 32395313 Free PMC article. Review.
Cited by
-
Effect of Elevated Neutrophil-to-Lymphocyte Ratio on Adverse Outcomes in Patients With Myocardial Infarction: A Systematic Review and Meta-Analysis.Cureus. 2024 Jun 4;16(6):e61647. doi: 10.7759/cureus.61647. eCollection 2024 Jun. Cureus. 2024. PMID: 38966451 Free PMC article. Review.
-
The predictive value of machine learning for mortality risk in patients with acute coronary syndromes: a systematic review and meta-analysis.Eur J Med Res. 2023 Oct 20;28(1):451. doi: 10.1186/s40001-023-01027-4. Eur J Med Res. 2023. PMID: 37864271 Free PMC article.
-
Construction and validation of a personalized risk prediction model for in-hospital mortality in patients with acute myocardial infarction undergoing percutaneous coronary intervention.Clinics (Sao Paulo). 2025 Feb 1;80:100580. doi: 10.1016/j.clinsp.2025.100580. eCollection 2025. Clinics (Sao Paulo). 2025. PMID: 39893830 Free PMC article.
-
Adherence to outpatient cardiac rehabilitation and related factors in STEMI after PCI in China: a sequential explanatory mixed method study protocol.Front Cardiovasc Med. 2025 Aug 5;12:1542942. doi: 10.3389/fcvm.2025.1542942. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40837241 Free PMC article.
-
ANMCO (Italian Association of Hospital Cardiologists) scientific statement: obesity in adults-an approach for cardiologists.Eat Weight Disord. 2024 Jan 2;29(1):1. doi: 10.1007/s40519-023-01630-8. Eat Weight Disord. 2024. PMID: 38168872 Free PMC article. Review.
References
-
- O'Gara PT, Kushner FG, Ascheim DD, et al. . 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of cardiology Foundation/American heart association Task force on practice guidelines. Circulation 2013;127:e362–425. 10.1161/CIR.0b013e3182742cf6 - DOI - PubMed
-
- Authors/Task Force Members, Piepoli MF, Hoes AW, et al. . 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts): Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur J Prev Cardiol 2016;23:NP1–-NP96. 10.1177/2047487316653709 - DOI - PubMed
-
- Ibanez B, James S, Agewall S, et al. . 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of cardiology (ESC). Eur Heart J 2018;39:119–77. 10.1093/eurheartj/ehx393 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous