

Phase Ib Trial of the Combination of Imatinib and Binimetinib in Patients with Advanced Gastrointestinal Stromal Tumors
- PMID: 35110417
- PMCID: PMC9012681
- DOI: 10.1158/1078-0432.CCR-21-3909
Phase Ib Trial of the Combination of Imatinib and Binimetinib in Patients with Advanced Gastrointestinal Stromal Tumors
Abstract
Purpose: This phase Ib trial was designed to evaluate the safety and early efficacy signal of the combination of imatinib and binimetinib in patients with imatinib-resistant advanced gastrointestinal stromal tumors (GISTs).
Patients and methods: This trial used a standard 3 + 3 design to determine the recommended phase II dose (RP2D). Additional patients were enrolled on an expansion cohort at the RP2D enriching for succinate dehydrogenase (SDH)-deficient GISTs to explore potential efficacy.
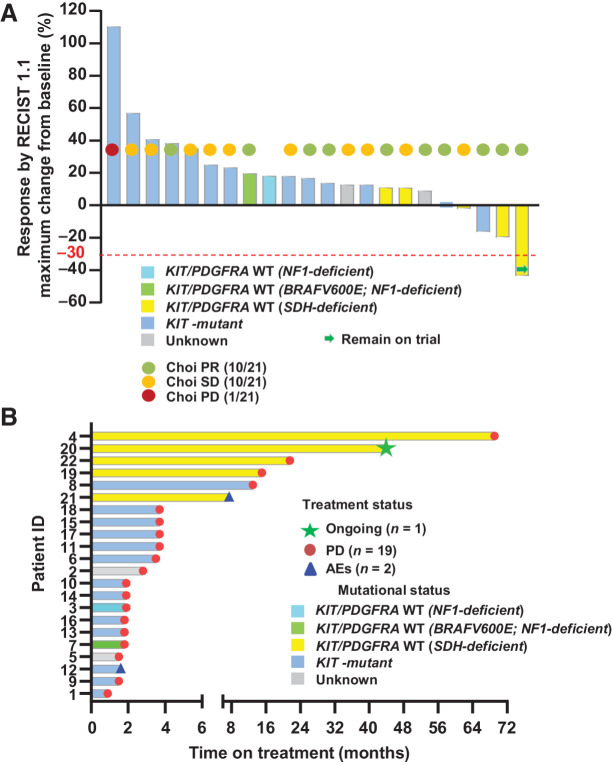
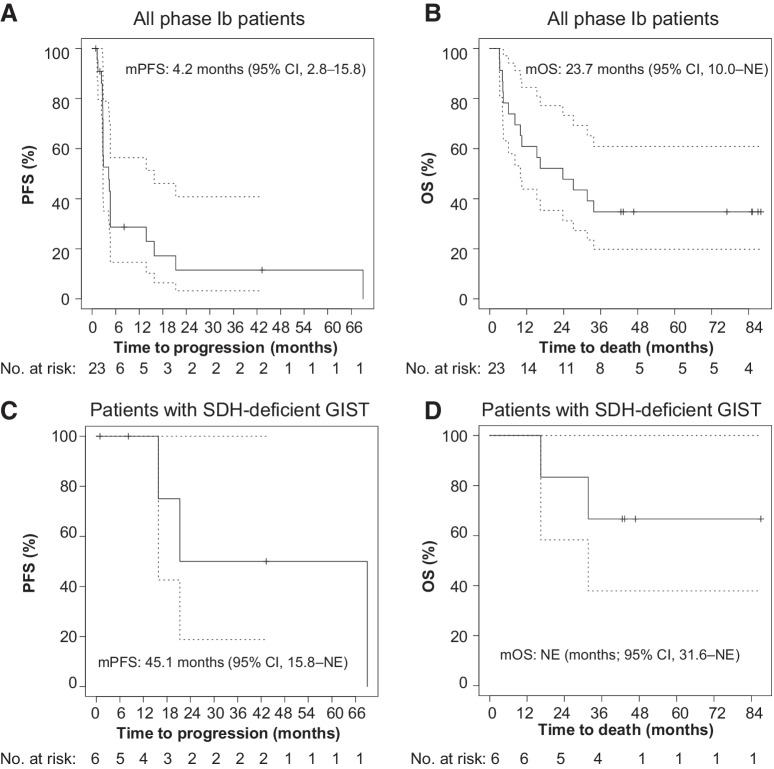
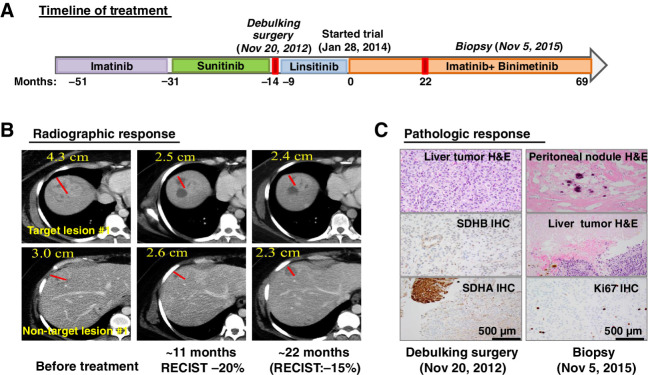
Results: The trial enrolled nine patients in the dose-escalation cohort and 14 in the dose-expansion cohort including six with SDH-deficient GISTs. Imatinib 400 mg daily with binimetinib 45 mg twice daily was established as the RP2D. Dose-limiting toxicity (DLT) was asymptomatic grade 4 creatinine phosphokinase (CPK) elevation. The most common non-DLT grade 3/4 toxicity was asymptomatic CPK elevation (69.6%). Other common ≥grade 2 toxicities included peripheral edema (17.4%), acneiform rash (21.7%), anemia (30.4%), hypophosphatemia (39.1%), and aspartate aminotransferase (AST) increase (17.4%). Two serious adverse events occurred (grade 2 dropped head syndrome and grade 3 central retinal vein occlusion). No unexpected toxicities were observed. Limited clinical activity was observed in KIT-mutant GIST. For SDH-deficient GISTs, one of five had confirmed RECIST1.1 partial response (PR). The median progression-free survival (mPFS) in patients with SDH-deficient GIST was 45.1 months [95% confidence interval (CI), 15.8-not estimable (NE)]; the median overall survival (mOS) was not reached (95% CI, 31.6 months-NE). One patient with a refractory metastatic SDH-deficient GIST had an exceptional pathologic response and durable clinical benefit.
Conclusions: The combination of imatinib and binimetinib is safe with manageable toxicity and has encouraging activity in SDH-deficient but not imatinib-refractory KIT/PDGFRA-mutant GISTs. The observed clinical benefits provide a motivation for a larger trial of the combination strategy in SDH-deficient GISTs.
Trial registration: ClinicalTrials.gov NCT01623349.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures

Comment in
- Clin Cancer Res. 28:1475.
References
-
- Corless CL, Barnett CM, Heinrich MC. Gastrointestinal stromal tumours: origin and molecular oncology. Nat Rev Cancer 2011;11:865–78. - PubMed
-
- Heinrich MC, Corless CL, Duensing A, McGreevey L, Chen CJ, Joseph N, et al. PDGFRA activating mutations in gastrointestinal stromal tumors. Science 2003;299:708–10. - PubMed
-
- Hirota S, Isozaki K, Moriyama Y, Hashimoto K, Nishida T, Ishiguro S, et al. Gain-of-function mutations of c-kit in human gastrointestinal stromal tumors. Science 1998;279:577–80. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01 CA252048/CA/NCI NIH HHS/United States
- P50 CA240243/CA/NCI NIH HHS/United States
- R01 CA228216/CA/NCI NIH HHS/United States
- P50 CA217694/CA/NCI NIH HHS/United States
- R01 FD005731/FD/FDA HHS/United States
- R35 CA197588/CA/NCI NIH HHS/United States
- DP2 CA174499/CA/NCI NIH HHS/United States
- K08 CA151660/CA/NCI NIH HHS/United States
- P50 CA140146/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- P50 CA168504/CA/NCI NIH HHS/United States
- R01 FD005105/FD/FDA HHS/United States
- R01 CA226776/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
