

Indolent enhancing spinal lesions mimicking spinal metastasis in pediatric patients with malignant primary brain tumors
- PMID: 35110660
- PMCID: PMC8811062
- DOI: 10.1038/s41598-022-05831-6
Indolent enhancing spinal lesions mimicking spinal metastasis in pediatric patients with malignant primary brain tumors
Abstract
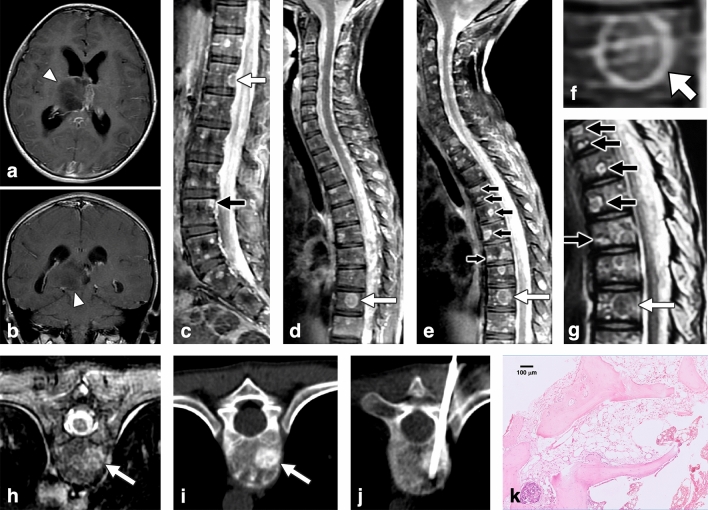
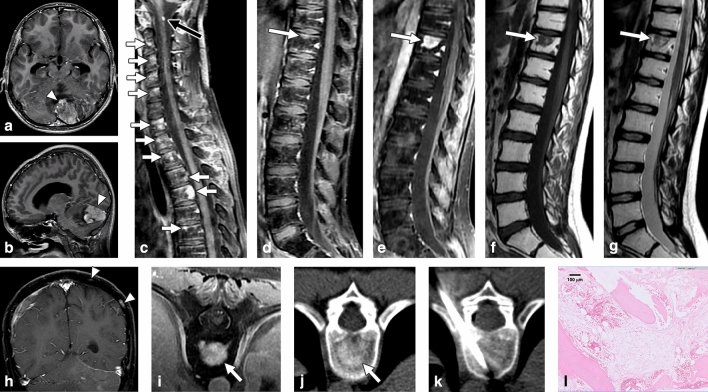
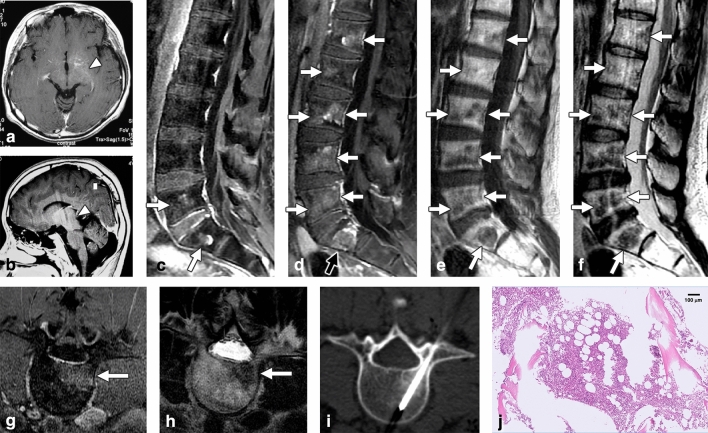
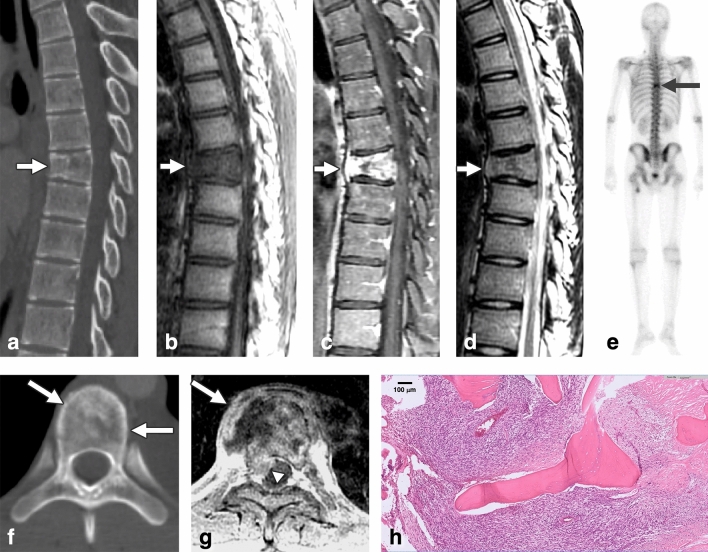
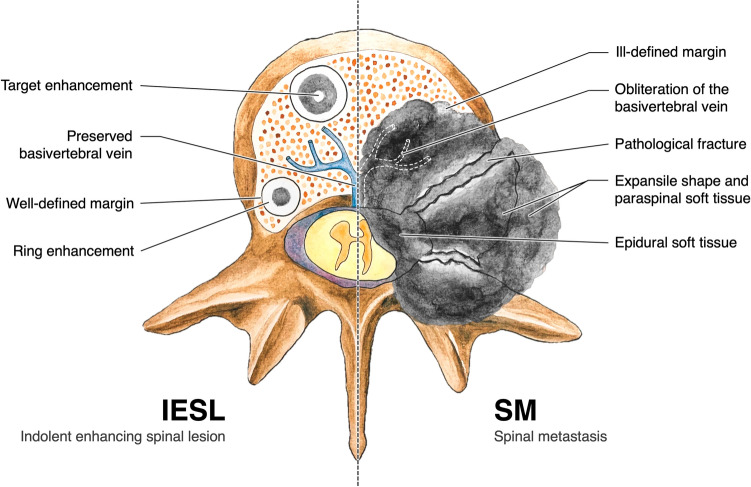
Spinal metastasis from malignant primary brain tumors (MPBTs) in pediatric patients is rare and often appears as enhancing lesions on MRI. However, some indolent enhancing spinal lesions (IESLs) resulting from previous treatment mimic metastasis on MRI, leading to unnecessary investigation and treatment. In 2005-2020, we retrospectively enrolled 12 pediatric/young patients with clinical impression of spinal metastasis and pathological diagnosis of their spinal lesions. Three patients had MPBT with IESL, and 9 patients had malignant tumors with metastases. The histopathologic diagnosis of IESL was unremarkable marrow change. We evaluated their MRI, CT, and bone scan findings. The following imaging findings of IESL vs. spinal metastasis were noted: (1) IESLs appeared round/ovoid (3/3, 100%), whereas spinal metastasis appeared irregular (9/9, 100%) (P = 0.005); (2) target-shaped enhancement was noted in (3/3, 100%) vs. (0/9, 0%) of cases, respectively (P = 0.005); (3) pathologic fracture of the vertebral body was noted in (1/3, 33.3%) vs. (9/9, 100%) of cases, respectively (P = 0.045); (4) expansile vertebral shape was noted in (0/3, 0%) vs. (9/9, 100%) of cases, respectively (P = 0.005); (5) obliteration of the basivertebral vein was noted in (0/3, 0%) vs. (9/9, 100%) of cases, respectively (P = 0.005); and (6) osteoblastic change on CT was noted in (3/3, 100%) vs. (2/9, 22.2%) of cases, respectively (P = 0.034). IESL in pediatric patients with MPBT can be differentiated from metastasis based on their imaging characteristics. We suggest close follow-up rather than aggressive investigation and treatment for IESL.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
