Management of Frontal Bone Fracture in a Tertiary Neurosurgical Care Center-A Retrospective Study
- PMID: 35110921
- PMCID: PMC8803529
- DOI: 10.1055/s-0041-1740615
Management of Frontal Bone Fracture in a Tertiary Neurosurgical Care Center-A Retrospective Study
Abstract
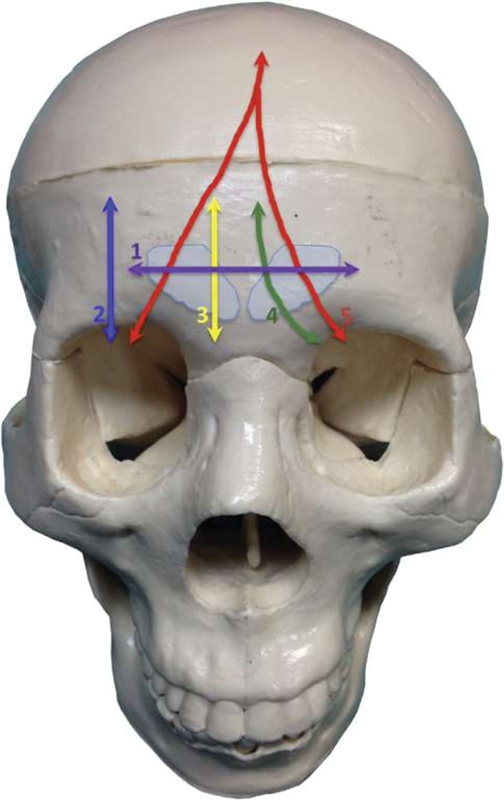
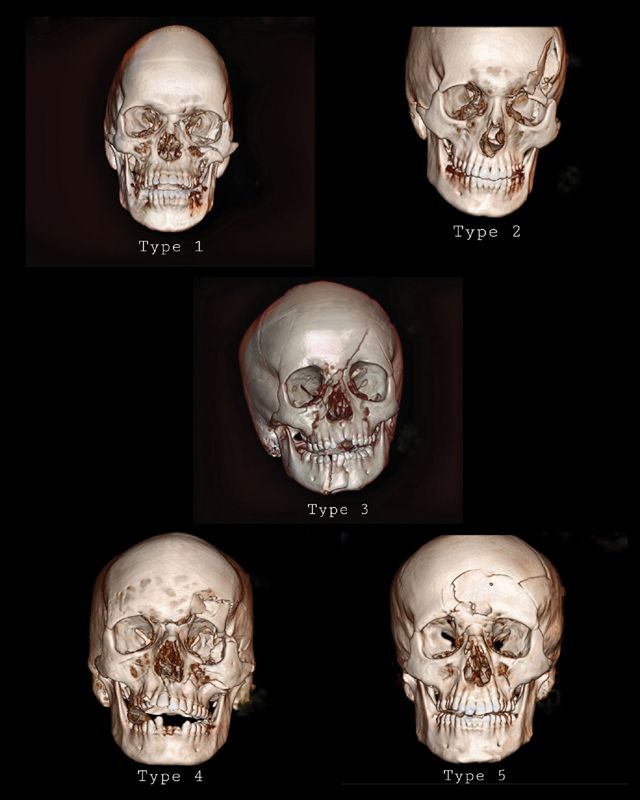
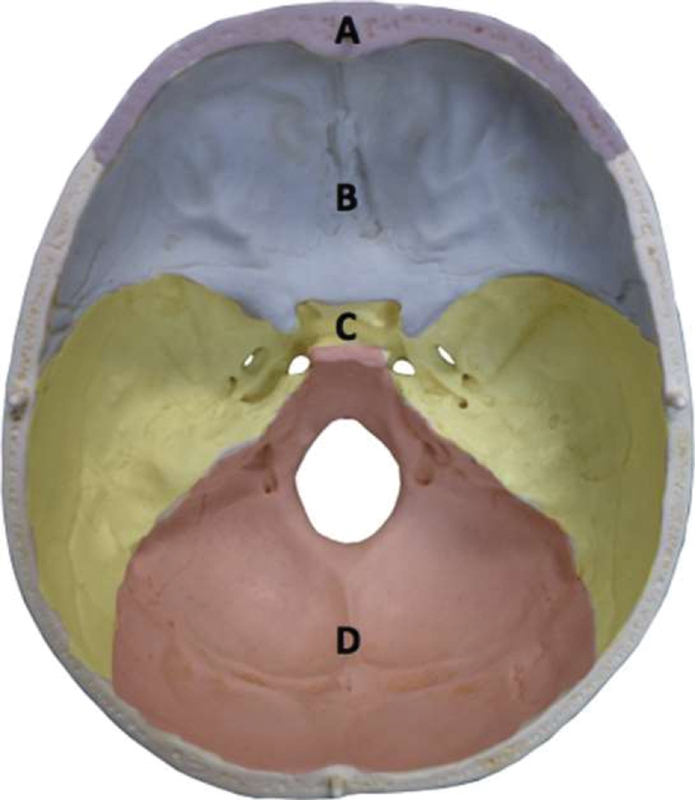
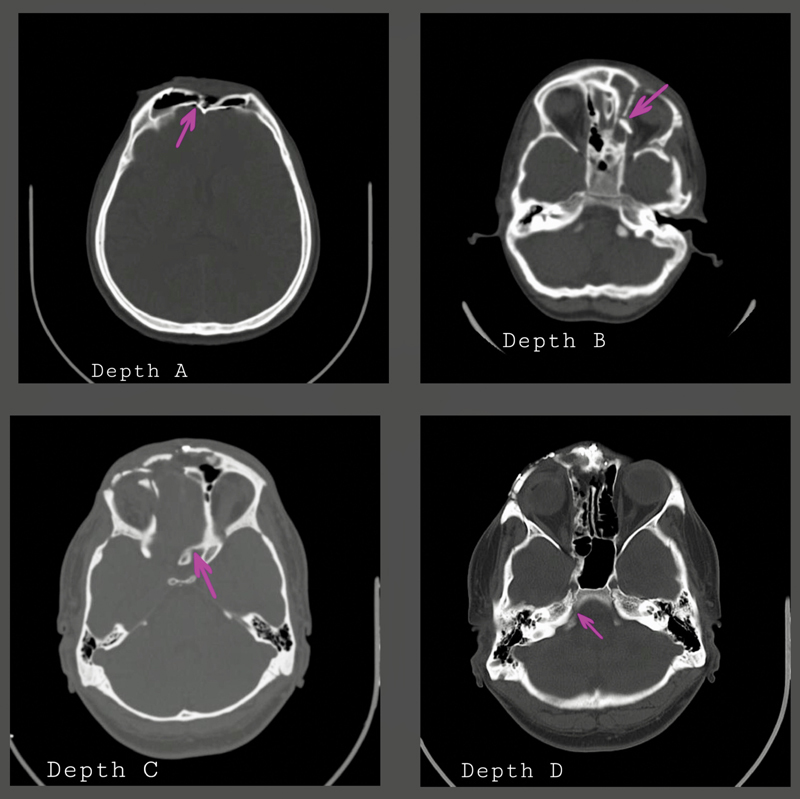
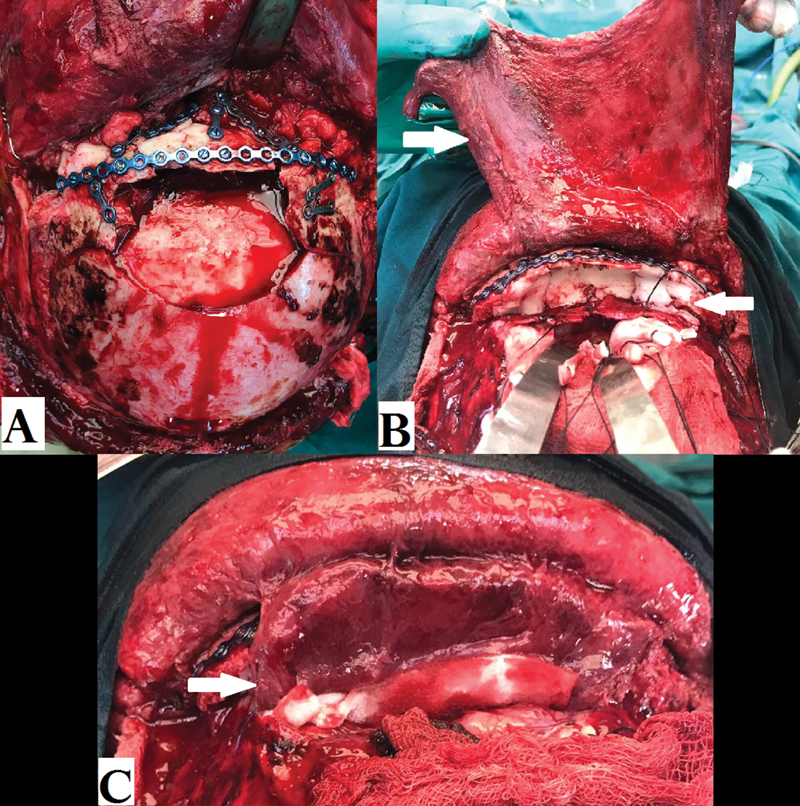
Objective We present our experience in the management of frontal bone fractures using the previously described radiologic classification of frontal bone fractures. Methodology A retrospective study was conducted, which reviewed the medical records and computed tomographic (CT) scan images of patients with frontal bone fracture from January 2016 to February 2019. Patients with complete medical records and a follow-up of minimum 1 year were included in the study. Demographic details, mechanism of injury, associated intracranial injuries, maxillofacial fractures, management, and complications were analyzed. CT scan images were used to classify the frontal bone fractures using the novel classification given by Garg et al (2014). The indications for surgical treatment were inner table frontal sinus fracture with cerebrospinal fluid (CSF) leak, intracranial hematoma with significant mass effect requiring surgical evacuation, and outer table comminuted fracture that is either causing nasofrontal duct obstruction or for cosmetic purpose. Results A total of 55 patients were included in the study. Road traffic accidents as the commonest cause of frontal bone fractures. The most common fracture pattern was type 1 followed by type 5 and depth B followed by depth A. Four patients presented with CSF rhinorrhea. CSF rhinorrhea was more frequent with fracture extension to the skull base (depth B, C, D), which was statistically significant ( p < 0.001). Conclusion Frontal bone fracture management has to be tailor-made for each patient based on the extent of the fracture, presence of CSF leak, and associated intracranial and maxillofacial injuries.
Keywords: CSF leak; cranialization; frontal bone fracture; frontal sinus fracture.
Association for Helping Neurosurgical Sick People. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures
Similar articles
-
Frontal Sinus Fractures: Management and Complications.Craniomaxillofac Trauma Reconstr. 2019 Sep;12(3):241-248. doi: 10.1055/s-0038-1675560. Epub 2019 Feb 19. Craniomaxillofac Trauma Reconstr. 2019. PMID: 31428249 Free PMC article.
-
A 10-year review of frontal sinus fractures: clinical outcomes of conservative management of posterior table fractures.Plast Reconstr Surg. 2012 Aug;130(2):399-406. doi: 10.1097/PRS.0b013e3182589d91. Plast Reconstr Surg. 2012. PMID: 22495212
-
Frontal Sinus Fractures: An Evaluation of Patient Demographics, Mechanisms of Injury, Classification, and Management Strategies in Patients Referred to a Trauma Center, From 2014 to 2019.J Craniofac Surg. 2024 Mar-Apr 01;35(2):505-509. doi: 10.1097/SCS.0000000000009786. Epub 2023 Oct 30. J Craniofac Surg. 2024. PMID: 37902320
-
Management of frontal sinus fractures. Changing concepts.Clin Plast Surg. 1992 Jan;19(1):219-32. Clin Plast Surg. 1992. PMID: 1537220 Review.
-
Surgical treatment of traumatic injuries of the cranial base.Otolaryngol Clin North Am. 2013 Oct;46(5):749-57. doi: 10.1016/j.otc.2013.06.008. Otolaryngol Clin North Am. 2013. PMID: 24138735 Review.
Cited by
-
Primary reconstruction of depressed frontal bone fracture including cranialization of frontal sinus and repair of forehead skin: a case report and literature review.AME Case Rep. 2025 Jul 11;9:92. doi: 10.21037/acr-2025-85. eCollection 2025. AME Case Rep. 2025. PMID: 40761200 Free PMC article.
References
-
- Maladière E, Bado F, Meningaud J P, Guilbert F, Bertrand J C. Aetiology and incidence of facial fractures sustained during sports: a prospective study of 140 patients. Int J Oral Maxillofac Surg. 2001;30(04):291–295. - PubMed