

Postmortem Biopsies of the Lung, Heart, Liver, and Spleen of COVID-19 Patients
- PMID: 35111427
- PMCID: PMC8792123
- DOI: 10.7759/cureus.20734
Postmortem Biopsies of the Lung, Heart, Liver, and Spleen of COVID-19 Patients
Abstract
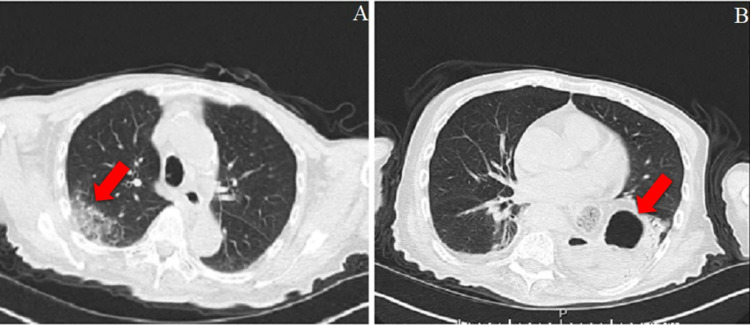
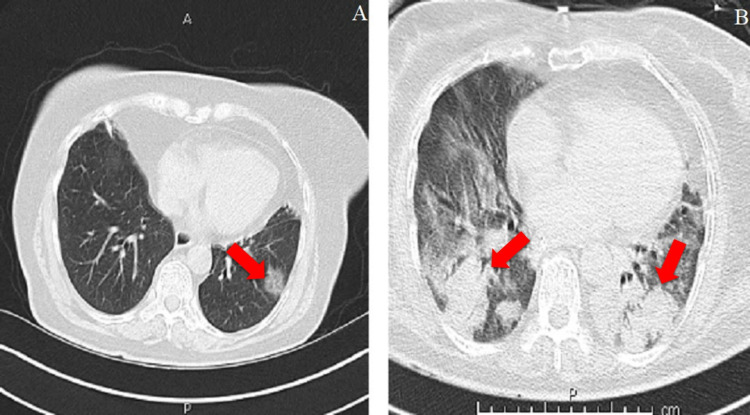
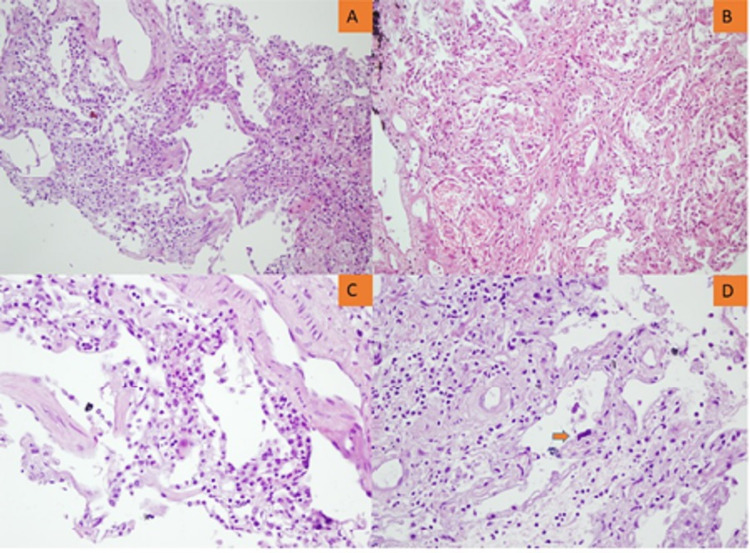
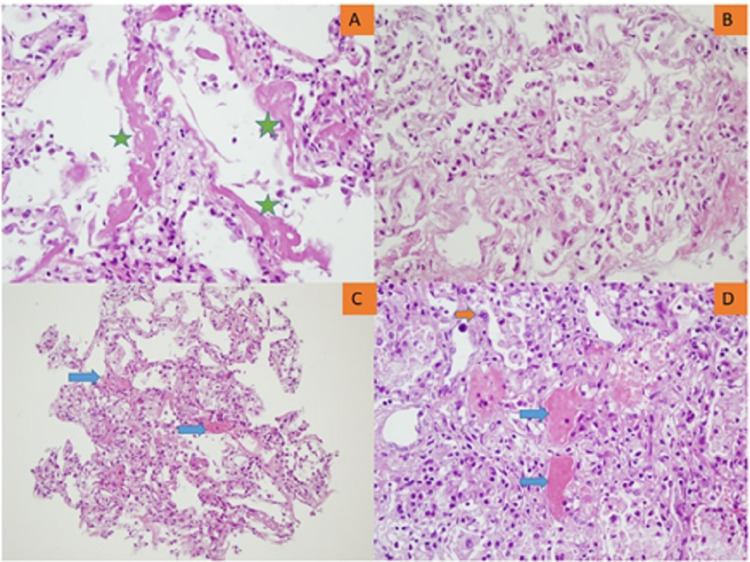
Objective We aimed to evaluate histopathologic alterations in the lung, heart, liver, and spleen of coronavirus disease 2019 (COVID-19) decedents through postmortem core needle biopsies. Materials and methods Patients who died of reverse transcription-polymerase chain reaction-proven COVID-19 were included in this postmortem case series. Postmortem percutaneous ultrasound-guided biopsies of the lungs, heart, liver, and spleen were performed using 14- and 16-gauge needles. Biopsy samples were stained with hematoxylin-eosin and examined under a light microscope. Clinicodemographic characteristics, chest computed tomography (CT) images, and COVID-19-related treatments of the patients were also collected. Results Seven patients were included in this study. Liver and heart tissue samples were available from all patients, and lung and spleen tissue samples were available from five and three patients, respectively. Chest CT images predominantly revealed bibasilar ground-glass opacities. Lung biopsies showed diffuse alveolar damage in all biopsy specimens. Heart findings were nonspecific and largely compatible with the underlying disease. Patchy necrosis, steatosis, and mononuclear cell infiltration were the main findings in the liver biopsies. Splenic histopathological examination showed that splenic necrosis and neutrophil infiltration were common findings in all patients. Conclusion Tissue acquisition was complete for the heart and liver and acceptable for the lungs. The amount of tissue was sufficient for a proper histopathologic examination. Histopathological findings were generally in accordance with previous autopsy studies. Radiological findings of the lung were also correlated with the histopathologic findings. We consider that a postmortem biopsy is a feasible alternative for histopathological examinations in COVID-19 decedents.
Keywords: biopsy; covid-19; heart; histopathologic; liver; lung; postmortem; sars-cov-2; spleen.
Copyright © 2021, Yurdaisik et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- The Johns Hopkins Coronavirus Resource Center. [ Aug; 2020 ];https://coronavirus.jhu.edu/map.html 2020
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous