

Scoring of medial arterial calcification predicts cardiovascular events and mortality after kidney transplantation
- PMID: 35112417
- PMCID: PMC9306575
- DOI: 10.1111/joim.13459
Scoring of medial arterial calcification predicts cardiovascular events and mortality after kidney transplantation
Abstract
Background: Progression of vascular calcification causes cardiovascular disease, which is the most common cause of death in chronic kidney failure and after kidney transplantation (KT). The prognostic impact of the extent of medial vascular calcification at KT is unknown.
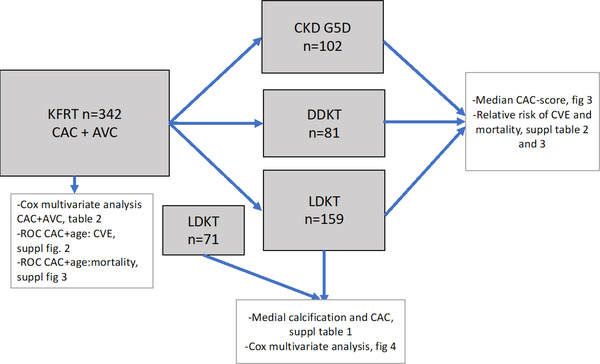
Methods: In this prospective cohort study, we investigated the impact of medial calcification compared to a mix of intimal and medial calcification represented by coronary artery calcification (CAC score) and aortic valve calcification in 342 patients starting on kidney failure replacement therapy. The primary outcomes were cardiovascular events (CVE) and death. The median follow-up time was 6.4 years (interquartile range 3.7-9.6 years). Exposure was CAC score and arteria epigastrica medial calcification scored as none, mild, moderate, or severe by a pathologist at time of KT (n = 200). We divided the patients according to kidney failure replacement therapy during follow-up, that is, living donor KT, deceased donor KT, or dialysis.
Results: Moderate to severe medial calcification in the arteria epigastrica was associated with higher mortality (p = 0.001), and the hazard ratio for CVE was 3.1 (95% confidence interval [CI] 1.12-9.02, p < 0.05) compared to no or mild medial calcification. The hazard ratio for 10-year mortality in the dialysis group was 33.6 (95% CI, 10.0-113.0, p < 0.001) compared to living donor recipients, independent of Framingham risk score and prevalent CAC.
Conclusion: Scoring of medial calcification in the arteria epigastrica identified living donor recipients as having 3.1 times higher risk of CVE, independent of traditional risk factors. The medial calcification score could be a reliable method to identify patients with high and low risk of CVE and mortality following KT.
Keywords: cardiovascular events; coronary artery calcification; kidney failure; medial calcification; mortality.
© 2022 The Authors. Journal of Internal Medicine published by John Wiley & Sons Ltd on behalf of Association for Publication of The Journal of Internal Medicine.
Conflict of interest statement
Peter Stenvinkel serves on scientific advisory boards for AstraZeneca, Baxter Healthcare, Reata Pharmaceuticals, Vifor, and Fresenius Medical Care. Annette Bruchfeld reports personal fees from AstraZeneca, Bayer, ChemoCentryx, and Vifor.
Figures



References
-
- Shanahan CM, Cary NR, Salisbury JR, Proudfoot D, Weissberg PL, Edmonds ME. Medial localization of mineralization‐regulating proteins in association with Monckeberg's sclerosis: evidence for smooth muscle cell‐mediated vascular calcification. Circulation. 1999;100:2168–76. 10.1161/01.cir.100.21.2168 - DOI - PubMed
