

Temsirolimus combined with cyclophosphamide and etoposide for pediatric patients with relapsed/refractory acute lymphoblastic leukemia: a Therapeutic Advances in Childhood Leukemia Consortium trial (TACL 2014-001)
- PMID: 35112552
- PMCID: PMC9521241
- DOI: 10.3324/haematol.2021.279520
Temsirolimus combined with cyclophosphamide and etoposide for pediatric patients with relapsed/refractory acute lymphoblastic leukemia: a Therapeutic Advances in Childhood Leukemia Consortium trial (TACL 2014-001)
Abstract
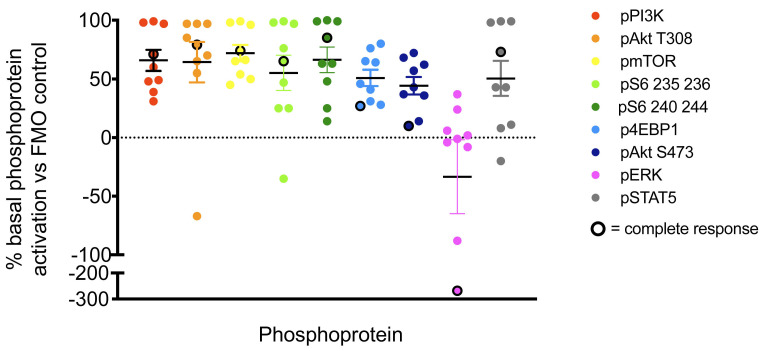
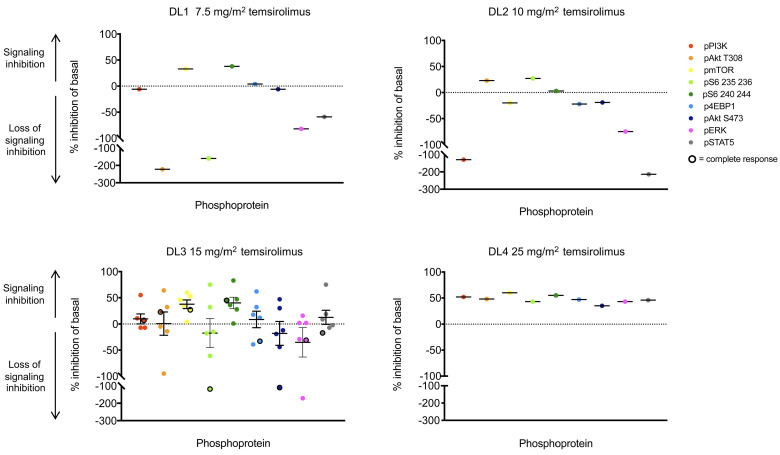
Phosphatidylinositol 3-kinase (PI3K)/mammalian target of rapamycin (mTOR) signaling is commonly dysregulated in acute lymphoblastic leukemia (ALL). The TACL2014-001 phase I trial of the mTOR inhibitor temsirolimus in combination with cyclophosphamide and etoposide was performed in children and adolescents with relapsed/refractory ALL. Temsirolimus was administered intravenously (IV) on days 1 and 8 with cyclophosphamide 440 mg/m2 and etoposide 100 mg/m2 IV daily on days 1-5. The starting dose of temsirolimus was 7.5 mg/m2 (DL1) with escalation to 10 mg/m2 (DL2), 15 mg/m2 (DL3), and 25 mg/m2 (DL4). PI3K/mTOR pathway inhibition was measured by phosphoflow cytometry analysis of peripheral blood specimens from treated patients. Sixteen heavily-pretreated patients were enrolled with 15 evaluable for toxicity. One dose-limiting toxicity of grade 4 pleural and pericardial effusions occurred in a patient treated at DL3. Additional dose-limiting toxicities were not seen in the DL3 expansion or DL4 cohort. Grade 3/4 non-hematologic toxicities occurring in three or more patients included febrile neutropenia, elevated alanine aminotransferase, hypokalemia, mucositis, and tumor lysis syndrome and occurred across all doses. Response and complete were observed at all dose levels with a 47% overall response rate and 27% complete response rate. Pharmacodynamic correlative studies demonstrated dose-dependent inhibition of PI3K/mTOR pathway phosphoproteins in all studied patients. Temsirolimus at doses up to 25 mg/m2 with cyclophosphamide and etoposide had an acceptable safety profile in children with relapsed/refractory ALL. Pharmacodynamic mTOR target inhibition was achieved and appeared to correlate with temsirolimus dose. Future testing of next-generation PI3K/mTOR pathway inhibitors with chemotherapy may be warranted to increase response rates in children with relapsed/refractory ALL.
Figures
Comment in
-
How do mTOR inhibitors fit in the landscape of treatment for relapsed acute lymphoblastic leukemia?Haematologica. 2022 Oct 1;107(10):2292-2294. doi: 10.3324/haematol.2021.280395. Haematologica. 2022. PMID: 35112555 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
