

Renal Protection with SGLT2 Inhibitors: Effects in Acute and Chronic Kidney Disease
- PMID: 35113333
- PMCID: PMC8888485
- DOI: 10.1007/s11892-021-01442-z
Renal Protection with SGLT2 Inhibitors: Effects in Acute and Chronic Kidney Disease
Abstract
Purpose of review: This review offers a critical narrative evaluation of emerging evidence that sodium-glucose co-transporter-2 (SGLT2) inhibitors exert nephroprotective effects in people with type 2 diabetes.
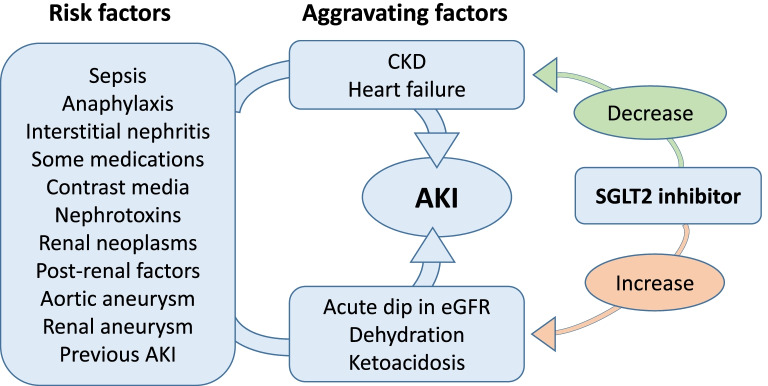
Recent findings: The SGLT2 inhibitor class of glucose-lowering agents has recently shown beneficial effects to reduce the onset and progression of renal complications in people with and without diabetes. Randomised clinical trials and 'real world' observational studies, mostly involving type 2 diabetes patients, have noted that use of an SGLT2 inhibitor can slow the decline in glomerular filtration rate (GFR), reduce the onset of microalbuminuria and slow or reverse the progression of proteinuria. The nephroprotective effects of SGLT2 inhibitors are class effects observed with each of the approved agents in people with a normal or impaired GFR. These effects are also observed in non-diabetic, lean and normotensive individuals suggesting that the mechanisms extend beyond the glucose-lowering, weight-lowering and blood pressure-lowering effects that accompany their glucosuric action in diabetes patients. A key mechanism is tubuloglomerular feedback in which SGLT2 inhibitors cause more sodium to pass along the nephron: the sodium is sensed by macula cells which act via adenosine to constrict afferent glomerular arterioles, thereby protecting glomeruli by reducing intraglomerular pressure. Other effects of SGLT2 inhibitors improve tubular oxygenation and metabolism and reduce renal inflammation and fibrosis. SGLT2 inhibitors have not increased the risk of urinary tract infections or the risk of acute kidney injury. However, introduction of an SGLT2 inhibitor in patients with a very low GFR is not encouraged due to an initial dip in GFR, and it is prudent to discontinue therapy if there is an acute renal event, hypovolaemia or hypotension.
Keywords: Acute kidney disease; Albuminuria; Chronic kidney disease; Diabetic kidney disease; Sodium-glucose co-transporter-2 (SGLT2) inhibitors.
© 2022. The Author(s).
Figures


References
-
- Wright EM, Loo DD, Hirayama BA. Biology of human sodium glucose transporters. Physiol Rev. 2011;91:733–794. - PubMed
-
- Bailey CJ. Renal glucose reabsorption inhibitors to treat diabetes. Trends Pharmacol Sci. 2011;32:63–71. - PubMed
-
- Ehrenkranz JR, Lewis NG, Kahn CR, Roth J. Phlorizin: a review. Diabetes Metab Res Rev. 2005;21:31–38. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
