

Current status of intra-cranial stereotactic radiotherapy and stereotactic radiosurgery in Australia and New Zealand: key considerations from a workshop and surveys
- PMID: 35113342
- PMCID: PMC8901507
- DOI: 10.1007/s13246-022-01108-4
Current status of intra-cranial stereotactic radiotherapy and stereotactic radiosurgery in Australia and New Zealand: key considerations from a workshop and surveys
Abstract
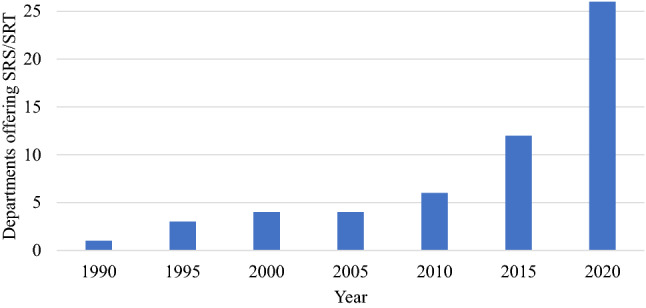
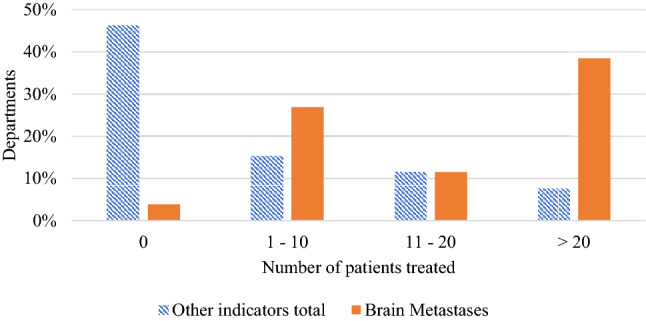
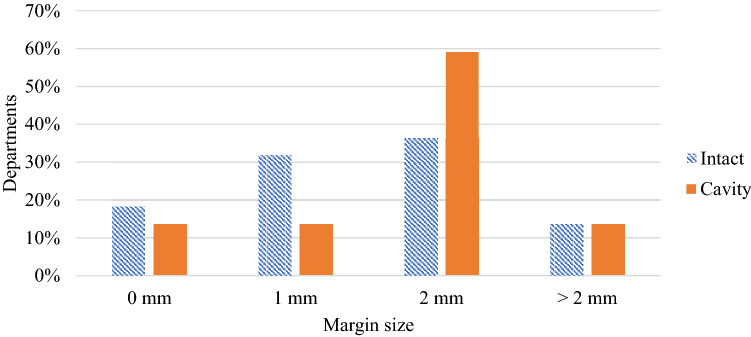
Recently, there has been increased interest worldwide in the use of conventional linear accelerator (linac)-based systems for delivery of stereotactic radiosurgery/radiotherapy (SRS/SRT) contrasting with historical delivery in specialised clinics with dedicated equipment. In order to gain an understanding and define the current status of SRS/SRT delivery in Australia and New Zealand (ANZ) we conducted surveys and provided a single-day workshop. Prior to the workshop ANZ medical physicists were invited to complete two surveys: a departmental survey regarding SRS/SRT practises and equipment; and an individual survey regarding opinions on current and future SRS/SRT practices. At the workshop conclusion, attendees completed a second opinion-based survey. Workshop discussion and survey data were utilised to identify areas of consensus, and areas where a community consensus was unclear. The workshop was held on the 8th Sept 2020 virtually due to pandemic-related travel restrictions and was attended by 238 radiation oncology medical physicists from 39 departments. The departmental survey received 32 responses; a further 89 and 142 responses were received to the pre-workshop and post-workshop surveys respectively. Workshop discussion indicated a consensus that for a department to offer an SRS/SRT service, a minimum case load should be considered depending on availability of training, peer-review, resources and equipment. It was suggested this service may be limited to brain metastases only, with less common indications reserved for departments with comprehensive SRS/SRT programs. Whilst most centres showed consensus with treatment delivery techniques and image guidance, opinions varied on the minimum target diameter and treatment margin that should be applied.
Keywords: Australia; New Zealand; Stereotactic radiosurgery; Stereotactic radiotherapy; Survey.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical