

A Systematic Review of Multi-decade Antibiotic Resistance Data for Ocular Bacterial Pathogens in the United States
- PMID: 35113406
- PMCID: PMC8927494
- DOI: 10.1007/s40123-021-00449-9
A Systematic Review of Multi-decade Antibiotic Resistance Data for Ocular Bacterial Pathogens in the United States
Abstract
Introduction: Since 2009, the Antibiotic Resistance Monitoring in Ocular Microorganisms (ARMOR) surveillance study has been assessing in vitro antibiotic resistance for bacterial isolates sourced from ocular infections in the US. The main goal of this systematic review was to compare in vitro resistance data for ocular pathogens from published US studies with the most recently published data from the ARMOR study (2009-2018) and, where possible, to evaluate trends in bacterial resistance over time over all studies.
Methods: A literature search was conducted using MEDLINE®, BIOSIS Previews®, and EMBASE® databases (1/1/1995-6/30/2021). Data were extracted from relevant studies and antibiotic susceptibility rates for common ocular pathogens (Staphylococcus aureus, coagulase-negative staphylococci [CoNS], Streptococcus pneumoniae, Pseudomonas aeruginosa, and Haemophilus influenzae), longitudinal changes in susceptibility, and multidrug resistance (MDR) were compared descriptively.
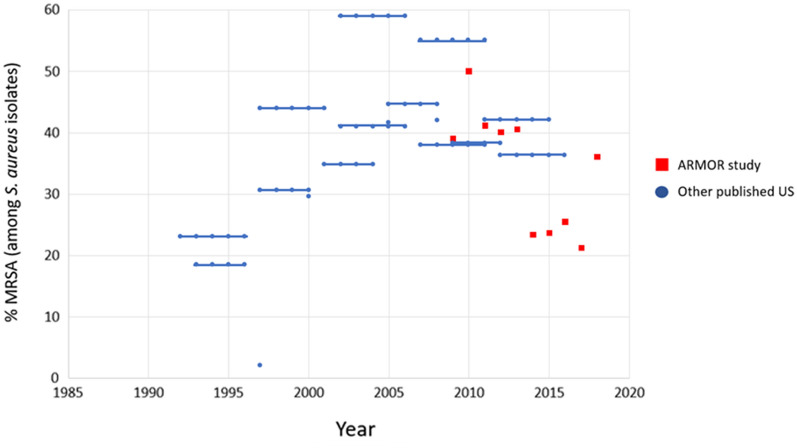
Results: Thirty-two relevant studies were identified. High in vitro resistance was found among S. aureus and CoNS to fluoroquinolones, macrolides, and methicillin/oxacillin across studies, with high rates of MDR noted, specifically among methicillin-resistant staphylococci. Data from studies pre-dating or overlapping the early years of ARMOR reflected increasing rates of S. aureus resistance to fluoroquinolones, macrolides, methicillin/oxacillin, and aminoglycosides, while the ARMOR data suggested slight decreases in resistance to these classes between 2009 and 2018. Overall, methicillin-resistant S. aureus (MRSA) prevalence peaked from 2005 to 2015 with a possible decreasing trend in more recent years.
Discussion and conclusions: Data from local and regional US datasets were generally consistent with data from the national ARMOR surveillance study. Continued surveillance of ocular bacterial pathogens is needed to track trends such as methicillin resistance and MDR prevalence and any new emerging antibiotic resistance phenotypes. Susceptibility data from ARMOR can inform initial choice of therapy, especially in practice areas where local antibiograms are unavailable.
Keywords: Antibiotic resistance; Conjunctivitis; Endophthalmitis; Keratitis; MRSA; Multidrug resistance; Ocular; Surveillance.
© 2022. The Author(s).
Figures

References
-
- Centers for Disease Control and Prevention. Antibiotic resistance: a global threat. 2020. https://www.cdc.gov/drugresistance/solutions-initiative/stories/ar-globa.... Accessed 11 May 2021.
-
- Lin A, Rhee MK, Akpek EK, et al. for the Cornea/External Disease Preferred Practice Panel 2017–2018. Bacterial Keratitis Preferred Practice Pattern®. American Academy of Ophthalmology; 2018.
Publication types
LinkOut - more resources
Full Text Sources
