

Pre-infection 25-hydroxyvitamin D3 levels and association with severity of COVID-19 illness
- PMID: 35113901
- PMCID: PMC8812897
- DOI: 10.1371/journal.pone.0263069
Pre-infection 25-hydroxyvitamin D3 levels and association with severity of COVID-19 illness
Retraction in
-
Retraction: Pre-infection 25-hydroxyvitamin D3 levels and association with severity of COVID-19 illness.PLoS One. 2025 Sep 8;20(9):e0331693. doi: 10.1371/journal.pone.0331693. eCollection 2025. PLoS One. 2025. PMID: 40920624 Free PMC article. No abstract available.
Abstract
Objective: Studies have demonstrated a potential correlation between low vitamin D status and both an increased risk of infection with SARS-CoV-2 and poorer clinical outcomes. This retrospective study examines if, and to what degree, a relationship exists between pre-infection serum 25-hydroxyvitamin D (25(OH)D) level and disease severity and mortality due to SARS-CoV-2.
Participants: The records of individuals admitted between April 7th, 2020 and February 4th, 2021 to the Galilee Medical Center (GMC) in Nahariya, Israel, with positive polymerase chain reaction (PCR) tests for SARS-CoV-2 (COVID-19) were searched for historical 25(OH)D levels measured 14 to 730 days prior to the positive PCR test.
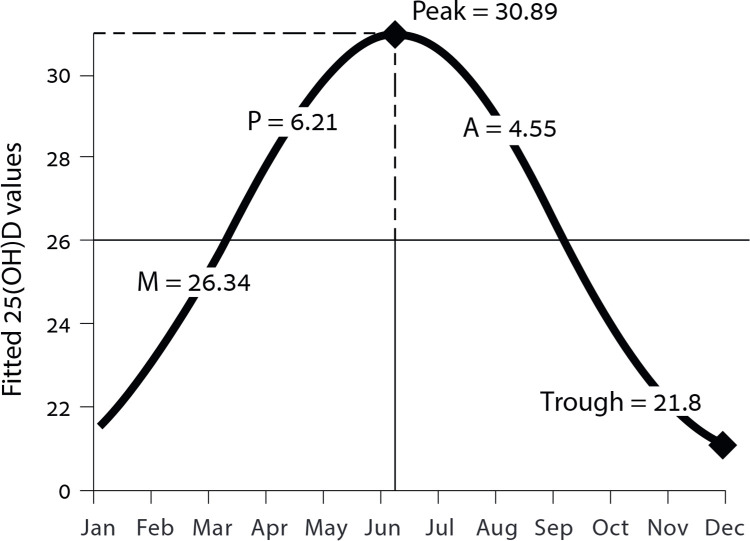
Design: Patients admitted to GMC with COVID-19 were categorized according to disease severity and level of 25(OH)D. An association between pre-infection 25(OH)D levels, divided between four categories (deficient, insufficient, adequate, and high-normal), and COVID-19 severity was ascertained utilizing a multivariable regression analysis. To isolate the possible influence of the sinusoidal pattern of seasonal 25(OH)D changes throughout the year, a cosinor model was used.
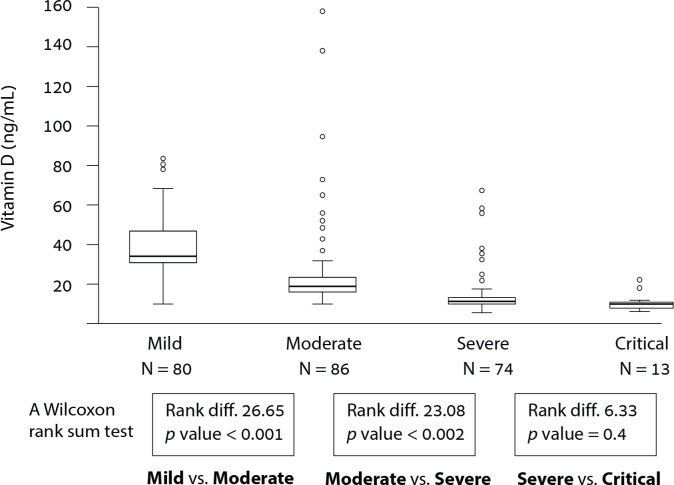
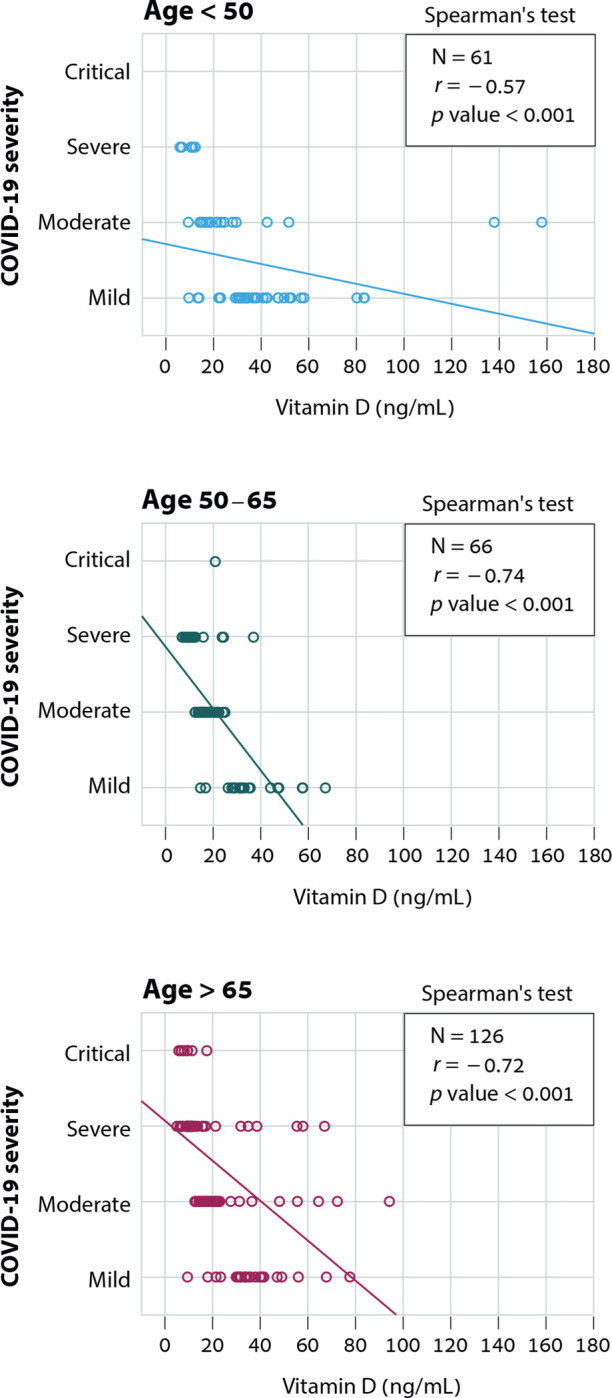
Results: Of 1176 patients admitted, 253 had records of a 25(OH)D level prior to COVID-19 infection. A lower vitamin D status was more common in patients with the severe or critical disease (<20 ng/mL [87.4%]) than in individuals with mild or moderate disease (<20 ng/mL [34.3%] p < 0.001). Patients with vitamin D deficiency (<20 ng/mL) were 14 times more likely to have severe or critical disease than patients with 25(OH)D ≥40 ng/mL (odds ratio [OR], 14; 95% confidence interval [CI], 4 to 51; p < 0.001).
Conclusions: Among hospitalized COVID-19 patients, pre-infection deficiency of vitamin D was associated with increased disease severity and mortality.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
