

The glymphatic hypothesis: the theory and the evidence
- PMID: 35115036
- PMCID: PMC8815211
- DOI: 10.1186/s12987-021-00282-z
The glymphatic hypothesis: the theory and the evidence
Abstract
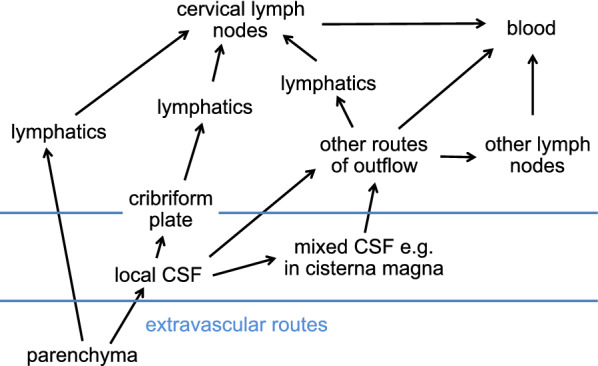
The glymphatic hypothesis proposes a mechanism for extravascular transport into and out of the brain of hydrophilic solutes unable to cross the blood-brain barrier. It suggests that there is a circulation of fluid carrying solutes inwards via periarterial routes, through the interstitium and outwards via perivenous routes. This review critically analyses the evidence surrounding the mechanisms involved in each of these stages. There is good evidence that both influx and efflux of solutes occur along periarterial routes but no evidence that the principal route of outflow is perivenous. Furthermore, periarterial inflow of fluid is unlikely to be adequate to provide the outflow that would be needed to account for solute efflux. A tenet of the hypothesis is that flow sweeps solutes through the parenchyma. However, the velocity of any possible circulatory flow within the interstitium is too small compared to diffusion to provide effective solute movement. By comparison the earlier classical hypothesis describing extravascular transport proposed fluid entry into the parenchyma across the blood-brain barrier, solute movements within the parenchyma by diffusion, and solute efflux partly by diffusion near brain surfaces and partly carried by flow along "preferred routes" including perivascular spaces, white matter tracts and subependymal spaces. It did not suggest fluid entry via periarterial routes. Evidence is still incomplete concerning the routes and fate of solutes leaving the brain. A large proportion of the solutes eliminated from the parenchyma go to lymph nodes before reaching blood but the proportions delivered directly to lymph or indirectly via CSF which then enters lymph are as yet unclear. In addition, still not understood is why and how the absence of AQP4 which is normally highly expressed on glial endfeet lining periarterial and perivenous routes reduces rates of solute elimination from the parenchyma and of solute delivery to it from remote sites of injection. Neither the glymphatic hypothesis nor the earlier classical hypothesis adequately explain how solutes and fluid move into, through and out of the brain parenchyma. Features of a more complete description are discussed. All aspects of extravascular transport require further study.
Keywords: Aquaporin 4; Blood–brain barrier; Bulk flow; Cerebrospinal; Diffusion; Extravascular transport; Fluid circulation; Glymphatic; Hydrophilic solute; Interstitial; Periarterial; Perivascular; Perivenous; Subependymal space.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- Abbott NJ, Pizzo ME, Preston JE, Janigro D, Thorne RG. The role of brain barriers in fluid movement in the CNS: is there a ‘glymphatic’ system? Acta Neuropathol. 2018;135:387–407. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
