

A scoring model combining serum alpha-fetoprotein and tumor size and number predicts prognosis in hepatitis B virus-related hepatocellular carcinoma patients after curative hepatectomy
- PMID: 35116886
- PMCID: PMC8798215
- DOI: 10.21037/tcr.2019.07.49
A scoring model combining serum alpha-fetoprotein and tumor size and number predicts prognosis in hepatitis B virus-related hepatocellular carcinoma patients after curative hepatectomy
Abstract
Background: More in-depth models, such as biomarker and anatomical information, are needed to predict individualized prognoses of hepatitis B virus (HBV)-related hepatocellular carcinoma (HCC) after curative liver resection. alpha-fetoprotein (AFP) has conflicting value in predicting prognosis. We aimed to investigate the significance of an AFP score model as a potential predictor of prognosis after radical resection in patients with HBV-related HCC.
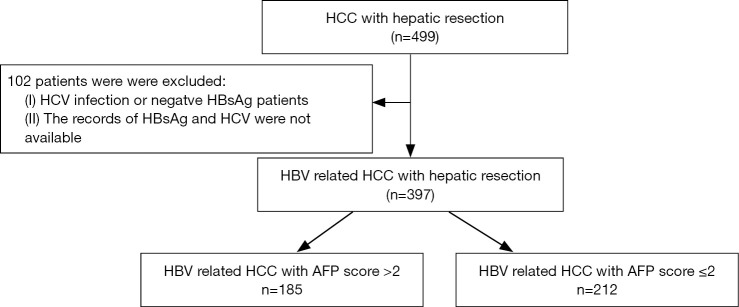
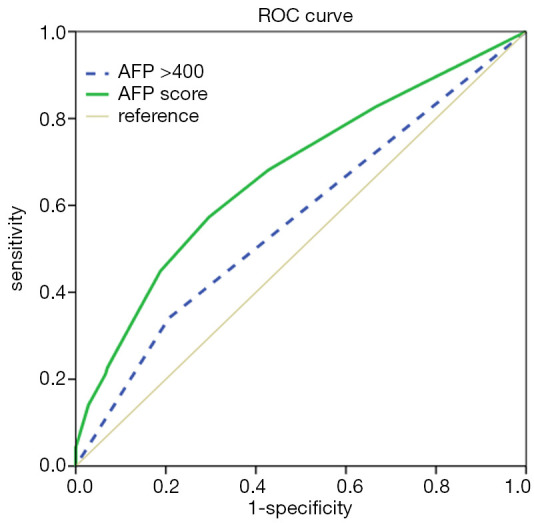
Methods: This study retrospectively analyzed 397 patients with HBV-related HCC who underwent hepatic resection between 2001 and 2013. Serum AFP level, tumor size, and tumor number were calculated by adding individual points for the AFP score model. Patient and tumor characteristics were tested for prognostic significance using ANOVA and chi-squared test, respectively. The receiver operating characteristic (ROC) curve was used to identify the AFP score model with or without other risk factors to discriminate patients. Kaplan-Meier and Cox's analyses were performed to pinpoint risk factors for overall survival (OS) and disease-free survival (DFS) in the patients.
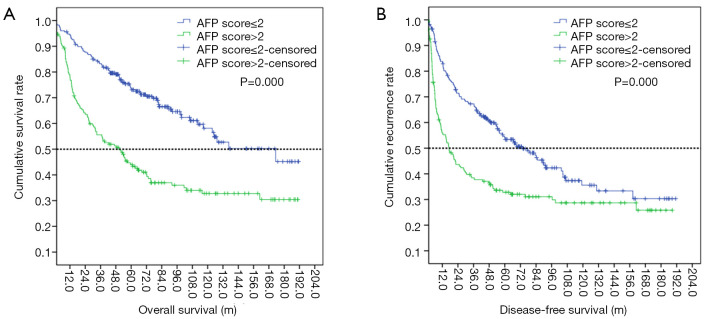
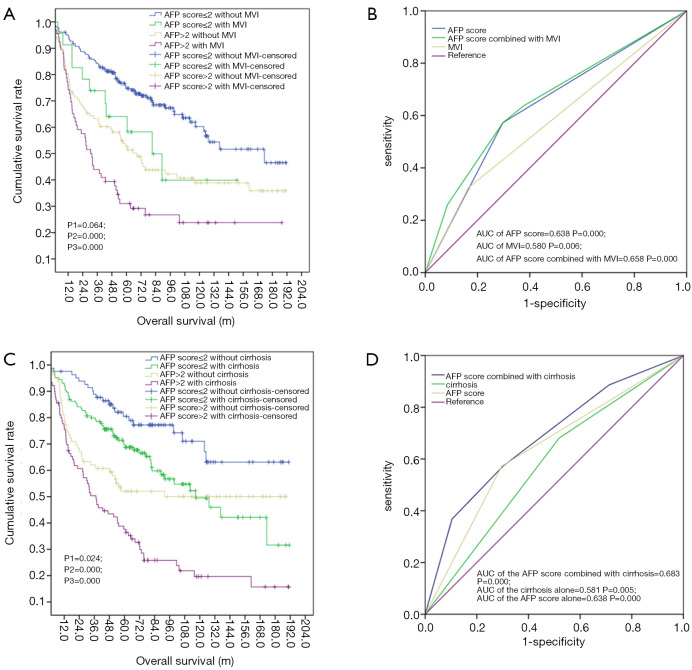
Results: The cutoff value for the AFP score model was set at 2 using the ROC curve, with good specificity and sensitivity for OS and DFS. According to the AFP score model, 185 patients were in the AFP score >2 group, and 212 were in the AFP score ≤2 group. The median OS in the AFP score ≤2 and AFP score >2 groups were 173.4±1.00 vs. 50.30±8.67 m, respectively (P=0.000). The median DFS in the AFP score ≤2 and AFP score >2 groups were 17.20±3.66 vs. 73.7±10.39 m (P=0.000), respectively. Analyses from Cox's multivariate proportional hazard model indicated that AFP score (HR =0.563, 95% CI: 0.398-0.798, P=0.001), MVI (HR =0.653, 95% CI: 0.441-0.967, P=0.033), and cirrhosis (HR =0.358, 95% CI: 0.185-0.696, P=0.002) were risk factors for OS. The multivariate Cox model identified MVI (HR =1.589, 95% CI: 1.496-2.854, P=0.003) and AFP score (HR =0.876, 95% CI: 0.404-0.925, P=0.040) as risk factors of DFS. According to the stratification by the AFP score with MVI, the mean OS in the AFP score >2 group combined with the MVI group was significantly shorter, compared with that in the AFP score >2 group without the MVI group (65.58±9.18 vs. 94.21±8.25 m, P=0.024). The mean OS in the AFP score >2 group combined with the cirrhosis group is significantly shorter than that in the AFP score ≤2 group without the cirrhosis group (64.08±7.38 vs. 145.31±8.38 m, P=0.000).
Conclusions: The AFP score model categorizes HCC patients with relatively good liver function after radical resection with low- and high-risk prognosis.
Keywords: AFP score model; Hepatocellular carcinoma (HCC); prognosis.
2019 Translational Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/tcr.2019.07.49). The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources