

Variant histology in bladder cancer: diagnostic and clinical implications
- PMID: 35117266
- PMCID: PMC8798576
- DOI: 10.21037/tcr-20-2169
Variant histology in bladder cancer: diagnostic and clinical implications
Abstract
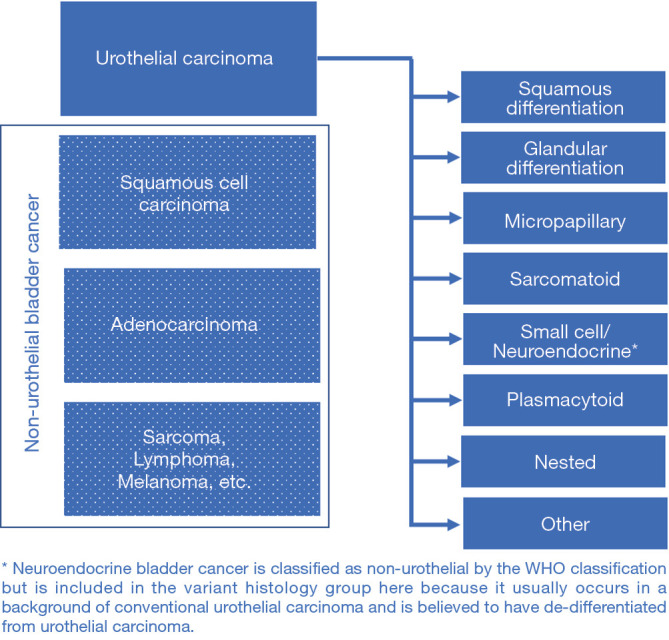
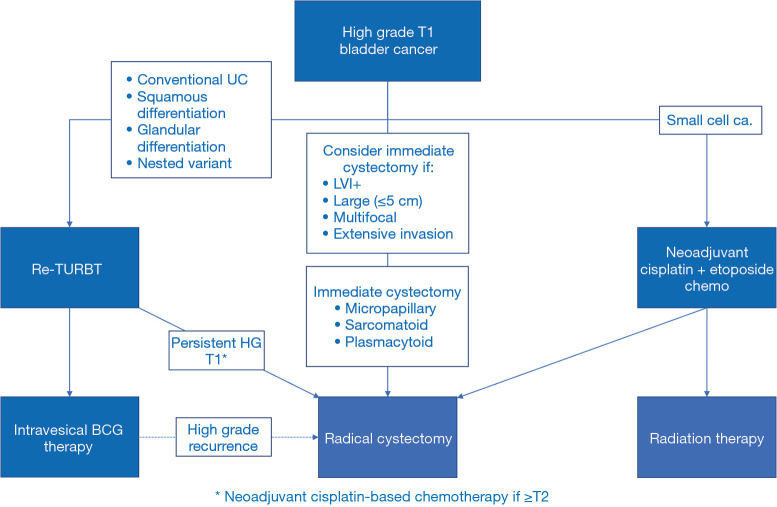
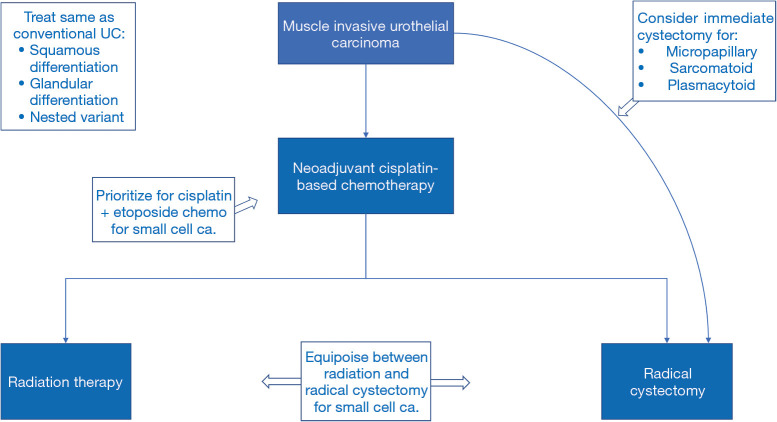
Urothelial carcinoma differentiates into variant histological subtypes in approximately 25% of cases. Since every histological variant has unique characteristics, including metastatic potential, expression of immunotherapy targets, and susceptibility to radiation or chemotherapy, every variant offers a unique diagnostic and therapeutic challenge. However, since any single variant is relatively rare, there is a risk of missed pathological diagnosis and sub-optimal clinical management. Ensuring awareness among pathologists and wide-spread familiarity with the nuances of variants among urologists is therefore essential. Additionally, variant histologies may act as an intermediate between classical clinicopathological staging of bladder cancer and evolving molecular classification. Therefore, this review aims to provide a brief overview of the diagnostic, prognostic, and therapeutic implications of each variant histologic subtype. Despite the development of standardized diagnostic criteria, the diagnosis of variant histologies continues to pose a challenge and results in significant interobserver variability. The prognosis of any single variant is poorly studied. However, squamous and glandular differentiation are thought to have little effect on prognosis while micropapillary, sarcomatoid, plasmacytoid, and small cell carcinomas are associated with a poor prognosis. Although evidence surrounding therapeutic strategies is sparse, management guidelines have been developed for variant histologies, which are often treated more aggressively than pure urothelial carcinoma. For example, the presence of variant histology warrants radical cystectomy in patients with T1 disease. Recommendations surrounding neo-adjuvant chemotherapy and radiation therapy also differ with each variant. As new treatments emerge for advanced bladder cancer, studying outcomes in each variant will become critical. Since prognosis and management hinge on the presence of variant histologies, accurate diagnosis and a thorough understanding of these variants are imperative for optimal management of urothelial carcinoma.
Keywords: Bladder cancer; diagnosis; prognosis; treatment; variant histology.
2020 Translational Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: Both authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/tcr-20-2169). The series “Urothelial Carcinoma” was commissioned by the editorial office without any funding or sponsorship. The authors have no other conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials