

Hysteroscopy in the management of endometrial hyperplasia and cancer in reproductive aged women: new developments and current perspectives
- PMID: 35117379
- PMCID: PMC8799018
- DOI: 10.21037/tcr-20-2092
Hysteroscopy in the management of endometrial hyperplasia and cancer in reproductive aged women: new developments and current perspectives
Abstract
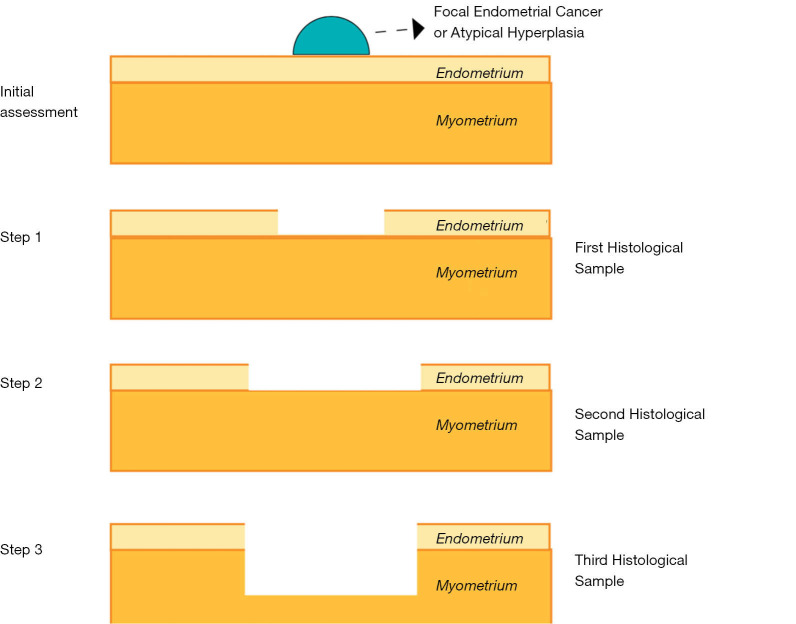
Over the last twenty years, the incidence of early endometrial cancer (EC) and atypical endometrial hyperplasia (AEH) among women of reproductive age is increasing rapidly, likely due to a combination of factors including increased prevalence of obesity and delayed of childbirths. Regarding preoperative diagnosis of endometrial neoplasia, it is still debated which is the most accurate and reliable method to obtain endometrial histopathological samples with fractional dilatation and curettage (D&C) having been considered, for a long time, as the method of choice. Nowadays, the advent of in-office endometrial biopsy with or without hysteroscopy has radically changed the approach, giving the opportunity to perform the endometrial biopsy under direct visualization. However, the lack of agreement about its diagnostic accuracy is still relevant. Since a significant number of women with AEH and/or EC are of childbearing age, a fertility-sparing diagnostic and therapeutic approach should be considered in all cases. The feasibility, safety and efficacy of fertility-sparing strategies involving hysteroscopic focal resections in conjunction with hormonal therapies have been evaluated and beneficial effects have been confirmed in several studies and one meta-analysis. Both local and systemic administration of hormonal therapies are currently used. Oral progestin, including medroxyprogesterone acetate (MPA) and megestrol acetate, are the most commonly used therapies. Nowadays, new therapeutic approaches, such as levonorgestrel intrauterine systems (LNG-IUS), gonadotropin-releasing hormone (GnRH) agonists, combined megestrol acetate and metformin, and other combinations of therapies are also used as first line therapies or after the hysteroscopic resection of the lesion. However, it is still unclear which approach provides higher clinical response with lower relapse rate, in addition to preserving fertility in women desiring to conceive. The aim of this narrative review is to summarize the available evidence regarding the evaluation and management with fertility-sparing treatments options of women with AEC and EC.
Keywords: Hysteroscopy; endometrial atypical hyperplasia; endometrial carcinoma; fertility-sparing; infertility.
2020 Translational Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/tcr-20-2092). The series “Endometrial Cancer” was commissioned by the editorial office without any funding or sponsorship. The authors have no other conflicts of interest to declare.
Figures
Similar articles
-
[GnRH-a combined fertility-sparing re-treatment in women with endometrial carcinoma or atypical endomertial hyperplasia who failed to oral progestin therapy].Zhonghua Fu Chan Ke Za Zhi. 2021 Aug 25;56(8):561-568. doi: 10.3760/cma.j.cn112141-20210603-00298. Zhonghua Fu Chan Ke Za Zhi. 2021. PMID: 34420288 Chinese.
-
Hysteroscopic Resection in Fertility-Sparing Surgery for Atypical Hyperplasia and Endometrial Cancer: Safety and Efficacy.J Minim Invasive Gynecol. 2015 Nov-Dec;22(7):1178-82. doi: 10.1016/j.jmig.2015.06.004. Epub 2015 Jun 16. J Minim Invasive Gynecol. 2015. PMID: 26092080
-
Levonorgestrel-releasing intrauterine device plus metformin, or megestrol acetate plus metformin for fertility-sparing treatment of atypical endometrial hyperplasia and early endometrial carcinoma: a prospective, randomized, blind-endpoint design trial protocol.Reprod Health. 2022 Nov 4;19(1):206. doi: 10.1186/s12978-022-01513-8. Reprod Health. 2022. PMID: 36333773 Free PMC article.
-
Oral and intrauterine progestogens for atypical endometrial hyperplasia.Cochrane Database Syst Rev. 2018 Dec 4;12(12):CD009458. doi: 10.1002/14651858.CD009458.pub3. Cochrane Database Syst Rev. 2018. PMID: 30521671 Free PMC article.
-
Fertility-sparing management for endometrial cancer: review of the literature.Minerva Med. 2021 Feb;112(1):55-69. doi: 10.23736/S0026-4806.20.07072-X. Epub 2020 Nov 18. Minerva Med. 2021. PMID: 33205638 Review.
Cited by
-
Comparison of prognosis of patients with endometrial cancer after hysteroscopy versus dilatation and curettage: A multicenter retrospective study.Front Med (Lausanne). 2023 Jan 9;9:1097133. doi: 10.3389/fmed.2022.1097133. eCollection 2022. Front Med (Lausanne). 2023. PMID: 36698830 Free PMC article.
-
Comparative effects of different treatments based on the levonorgestrel intrauterine system in endometrial carcinoma and endometrial hyperplasia patients: a network meta-analysis.Arch Gynecol Obstet. 2024 Sep;310(3):1315-1329. doi: 10.1007/s00404-024-07608-w. Epub 2024 Jul 9. Arch Gynecol Obstet. 2024. PMID: 38980346 Review.
-
The role of hysteroscopy in fertility preservation in endometrial cancer and atypical endometrial hyperplasia: a semi-systematic literature review.Arch Gynecol Obstet. 2023 Oct;308(4):1113-1126. doi: 10.1007/s00404-023-06960-7. Epub 2023 Feb 19. Arch Gynecol Obstet. 2023. PMID: 36807742
-
Clinical, Sonographic, and Hysteroscopic Features of Endometrial Carcinoma Diagnosed after Hysterectomy in Patients with a Preoperative Diagnosis of Atypical Hyperplasia: A Single-Center Retrospective Study.Diagnostics (Basel). 2022 Dec 2;12(12):3029. doi: 10.3390/diagnostics12123029. Diagnostics (Basel). 2022. PMID: 36553034 Free PMC article.
-
Diagnosis and Prediction of Endometrial Carcinoma Using Machine Learning and Artificial Neural Networks Based on Public Databases.Genes (Basel). 2022 May 24;13(6):935. doi: 10.3390/genes13060935. Genes (Basel). 2022. PMID: 35741697 Free PMC article.
References
-
- Kurman RJ. WHO classification of tumours of female reproductive organs. Fourth edition. World Health Organization Classification of Tumours. - PubMed
-
- Carcangiu ML, Kurman RJ, Carcangiu ML, et al. WHO Classification of Tumours of Female Reproductive Organs. 4th ed. World Health Organization Classification of Tumours. Lyon: International Agency for Research on Cancer; 2014.
Publication types
LinkOut - more resources
Full Text Sources