

Advantages of Widefield Optical Coherence Tomography in the Diagnosis of Retinopathy of Prematurity
- PMID: 35118032
- PMCID: PMC8806029
- DOI: 10.3389/fped.2021.797684
Advantages of Widefield Optical Coherence Tomography in the Diagnosis of Retinopathy of Prematurity
Abstract
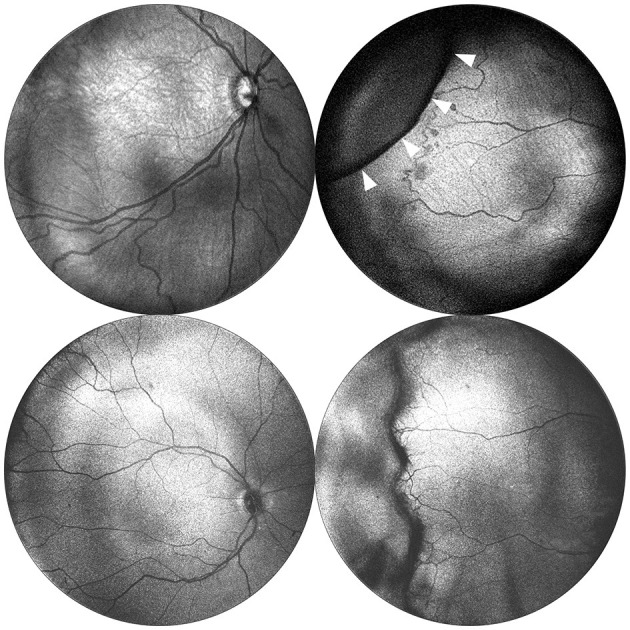
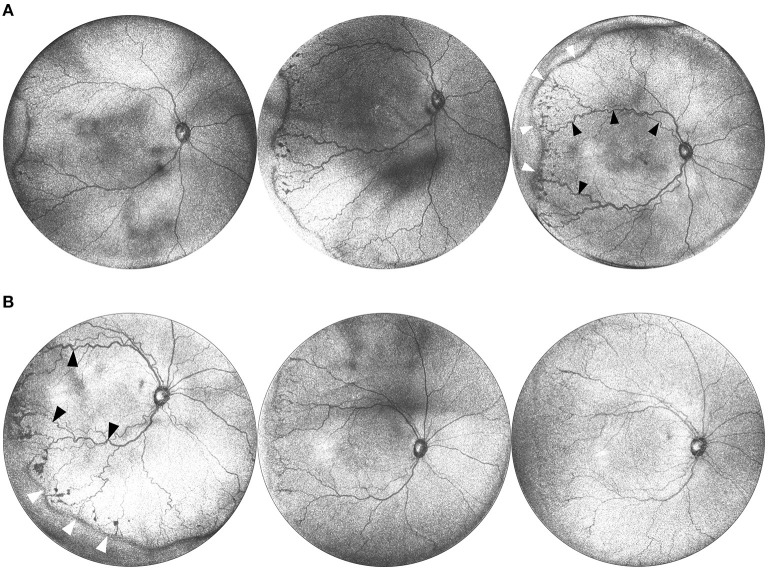
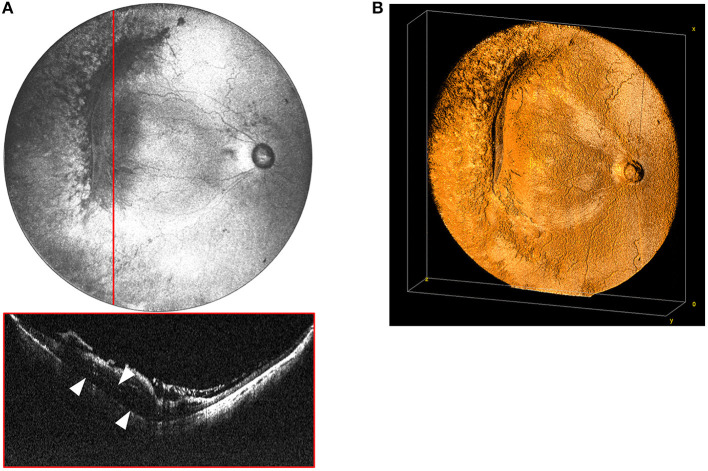
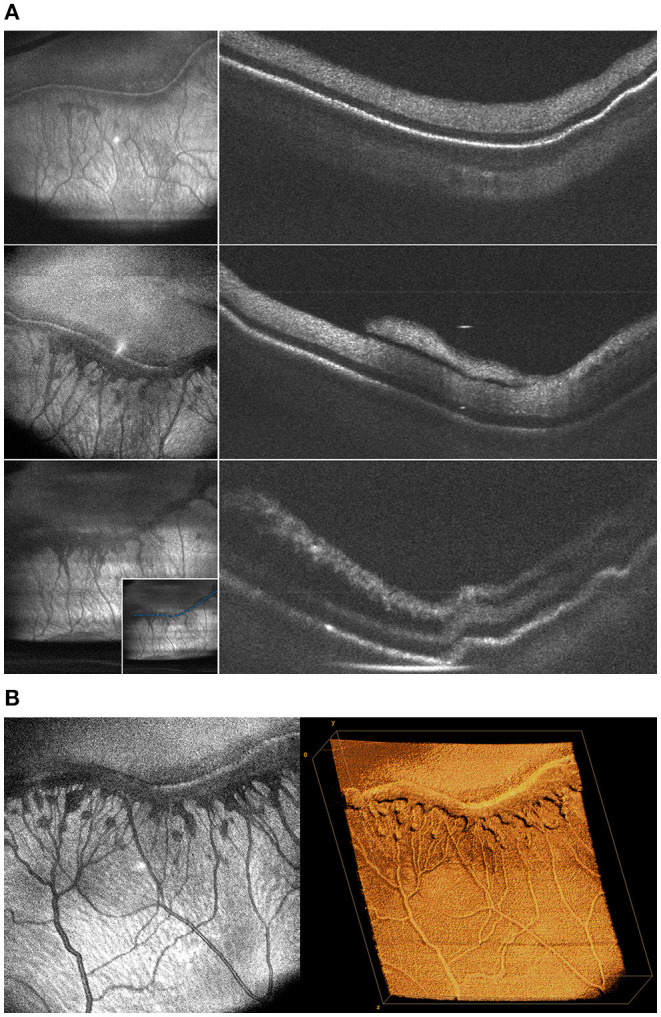
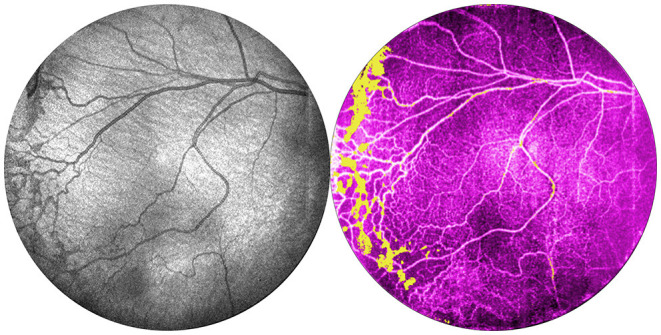
Recent advances in portable optical coherence tomography (OCT) and OCT angiography (OCTA) have resulted in wider fields of view (FOV) and shorter capture times, further expanding the potential clinical role of OCT technology in the diagnosis and management of retinopathy of prematurity (ROP). Using a prototype, handheld OCT device, retinal imaging was obtained in non-sedated infants in the neonatal intensive care unit (NICU) as well as sedated infants in the operating room of Oregon Health & Science University (OHSU) Hospital. In this observational study, we provide an overview of potential advantages of OCT-based disease assessment in ROP. We observed that next-generation OCT imaging (a) may be sufficient for objective diagnosis and zone/stage/plus disease categorization, (b) allows for minimally-invasive longitudinal monitoring of disease progression and post-treatment course, (c) provides three-dimensional mapping of the vitreoretinal interface, and (d) with OCTA, enables dye-free visualization of normal and pathologic vascular development.
Keywords: handheld optical coherence tomography; optical coherence tomography; optical coherence tomography with angiography; pediatric retina; retinopathy of prematurity.
Copyright © 2022 Nguyen, Ni, Khan, Wei, Ostmo, Chiang, Jia, Huang, Jian and Campbell.
Conflict of interest statement
Oregon Health & Science University (OHSU), DH, and YaJ have significant financial interests in Optovue, a company that may have a commercial interest in the results of this research and technology. These potential conflicts of interest have been reviewed and managed by OHSU. DH and YaJ have received royalties for patent files through OHSU, as well as loaned equipment for research from Optovue. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Vinekar A, Avadhani K, Sivakumar M, Mahendradas P, Kurian M, Braganza S, et al. . Understanding clinically undetected macular changes in early retinopathy of prematurity on spectral domain optical coherence tomography. Investig Ophthalmol Visual Sci. (2011) 52:5183–8. 10.1167/iovs.10-7155 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources