

Effects of norepinephrine infusion on cerebral energy metabolism during experimental haemorrhagic shock
- PMID: 35118520
- PMCID: PMC8814229
- DOI: 10.1186/s40635-022-00432-z
Effects of norepinephrine infusion on cerebral energy metabolism during experimental haemorrhagic shock
Abstract
Background: The use of norepinephrine in the case of life-threatening haemorrhagic shock is well established but widely discussed. The present study was designed to compare the effects of early norepinephrine treatment vs. no treatment on cerebral energy metabolism during haemorrhagic shock.
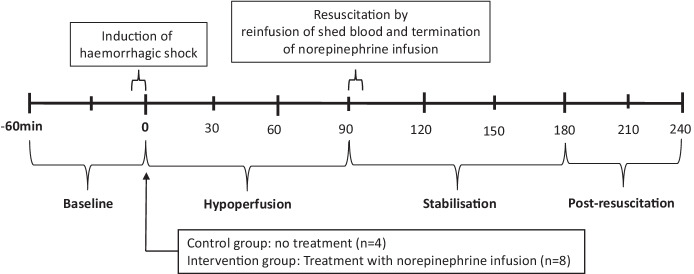
Methods: Twelve pigs were subjected to haemorrhagic shock, 4 in the control group and 8 in the norepinephrine (NE) group. Following a 60 min baseline period haemorrhagic shock was achieved by bleeding all animals to a pre-defined mean arterial blood pressure (MAP) of approximately 40 mm Hg. When mean arterial pressure had decreased to 40 mmHg NE infusion started in the treatment group. After 90 min, NE infusion stopped, and all pigs were resuscitated with autologous blood and observed for 2.5 h. During the experiment cerebral tissue oxygenation (PbtO2) was monitored continuously and variables reflecting cerebral energy metabolism (glucose, lactate, pyruvate, glutamate, glycerol) were measured by utilizing intracerebral microdialysis.
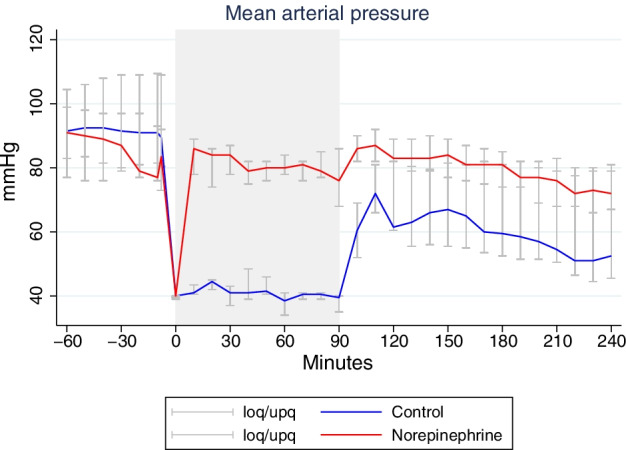
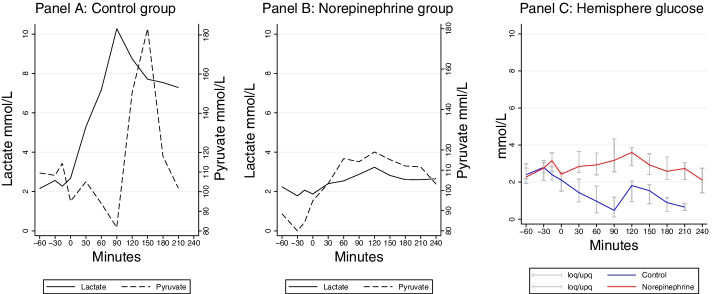
Results: All 12 pigs completed the protocol. NE infusion resulted in significantly higher MAP (p < 0.001). During the shock period lactate/pyruvate (LP) ratio group increased from 20 (15-29) to 66 (38-82) (median (IQR)) in the control group but remained within normal limits in the NE group. The significant increase in LP ratio in the control group remained after resuscitation. After induction of shock PbtO2 decreased markedly in the control group and was significantly lower than in the NE group during the resuscitation phase.
Conclusion: NE infusion during haemorrhagic shock improved cerebral energy metabolism compared with no treatment.
Keywords: Cerebral metabolism; Haemorrhagic shock; Microdialysis; Norepinephrine; Trauma.
© 2022. The Author(s).
Conflict of interest statement
Rasmus Peter Jakobsen, Elisabeth Charlotte Hansen, Troels Halfeld Nielsen, Carl-Henrik Nordström and Palle Toft declare that they have no competing interests.
Figures
Similar articles
-
Moderately prolonged permissive hypotension results in reversible metabolic perturbation evaluated by intracerebral microdialysis - an experimental animal study.Intensive Care Med Exp. 2019 Dec 4;7(1):67. doi: 10.1186/s40635-019-0282-x. Intensive Care Med Exp. 2019. PMID: 31802303 Free PMC article.
-
A technique for continuous bedside monitoring of global cerebral energy state.Intensive Care Med Exp. 2016 Dec;4(1):3. doi: 10.1186/s40635-016-0077-2. Epub 2016 Jan 20. Intensive Care Med Exp. 2016. PMID: 26791144 Free PMC article.
-
Regional and local brain oxygenation during hemorrhagic shock: a prospective experimental study on the effects of small-volume resuscitation with norepinephrine.J Trauma. 2008 Mar;64(3):641-8; discussion 648-9. doi: 10.1097/TA.0b013e3181637a6c. J Trauma. 2008. PMID: 18332803
-
Apelin-13 administration allows for norepinephrine sparing in a rat model of cecal ligation and puncture-induced septic shock.Intensive Care Med Exp. 2024 Aug 5;12(1):68. doi: 10.1186/s40635-024-00650-7. Intensive Care Med Exp. 2024. PMID: 39103658 Free PMC article.
-
Bedside interpretation of cerebral energy metabolism utilizing microdialysis in neurosurgical and general intensive care.Front Neurol. 2022 Aug 10;13:968288. doi: 10.3389/fneur.2022.968288. eCollection 2022. Front Neurol. 2022. PMID: 36034291 Free PMC article. Review.
Cited by
-
Low-dose norepinephrine in combination with hypotensive resuscitation may prolong the golden window for uncontrolled hemorrhagic shock in rats.Front Physiol. 2022 Sep 19;13:1004714. doi: 10.3389/fphys.2022.1004714. eCollection 2022. Front Physiol. 2022. PMID: 36200050 Free PMC article.
References
-
- Cecconi M, De Backer D, Antonelli M, Beale R, Bakker J, Hofer C, Jaeschke R, Mebazaa A, Pinsky MR, Teboul JL, Vincent JL, Rhodes A. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014;40:1795–1815. doi: 10.1007/s00134-014-3525-z. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
