

COVID-19 Vaccine Rollouts and the Reproduction of Urban Spatial Inequality: Disparities Within Large US Cities in March and April 2021 by Racial/Ethnic and Socioeconomic Composition
- PMID: 35118595
- PMCID: PMC8812364
- DOI: 10.1007/s11524-021-00589-0
COVID-19 Vaccine Rollouts and the Reproduction of Urban Spatial Inequality: Disparities Within Large US Cities in March and April 2021 by Racial/Ethnic and Socioeconomic Composition
Abstract
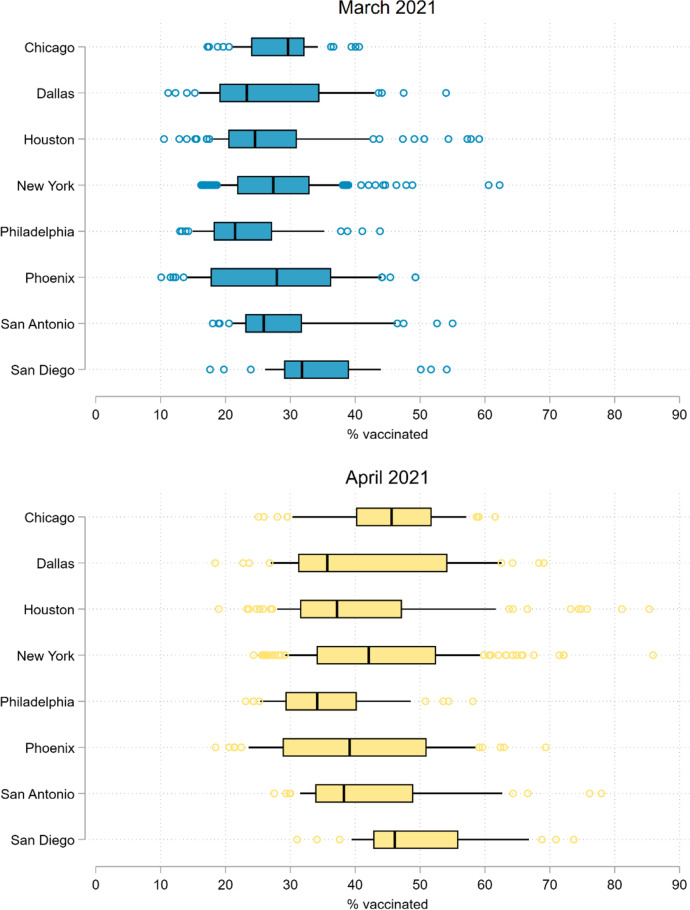
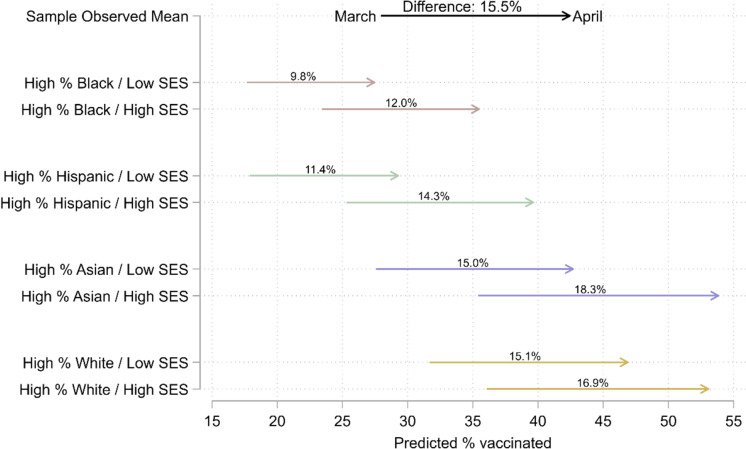
Rollouts of COVID-19 vaccines in the USA were opportunities to redress disparities that surfaced during the pandemic. Initial eligibility criteria, however, neglected geographic, racial/ethnic, and socioeconomic considerations. Marginalized populations may have faced barriers to then-scarce vaccines, reinforcing disparities. Inequalities may have subsided as eligibility expanded. Using spatial modeling, we investigate how strongly local vaccination levels were associated with socioeconomic and racial/ethnic composition as authorities first extended vaccine eligibility to all adults. We harmonize administrative, demographic, and geospatial data across postal codes in eight large US cities over 3 weeks in Spring 2021. We find that, although vaccines were free regardless of health insurance coverage, local vaccination levels in March and April were negatively associated with poverty, enrollment in means-tested public health insurance (e.g., Medicaid), and the uninsured population. By April, vaccination levels in Black and Hispanic communities were only beginning to reach those of Asian and White communities in March. Increases in vaccination were smaller in socioeconomically disadvantaged Black and Hispanic communities than in more affluent, Asian, and White communities. Our findings suggest vaccine rollouts contributed to cumulative disadvantage. Populations that were left most vulnerable to COVID-19 benefited least from early expansions in vaccine availability in large US cities.
Keywords: COVID-19; Disparities; Inequality; Neighborhood; Pandemic; Race; Socioeconomic; Spatial; Urban; Vaccine.
© 2022. The Author(s).
Figures
References
-
- Understanding vaccination progress. Johns Hopkins Coronavirus Resource Center. Accessed May 11, 2021. https://coronavirus.jhu.edu/vaccines/us-states
-
- Thompson MG. Interim estimates of vaccine effectiveness of BNT162b2 and mRNA-1273 COVID-19 vaccines in preventing SARS-CoV-2 infection among health care personnel, first responders, and other essential and frontline workers — eight U.S. locations, December 2020–March 2021. Morb Mortal Wkly Rep. 2021;70(13):495–500. doi: 10.15585/mmwr.mm7013e3. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
