

Programmed intermittent epidural bolus in parturients: A meta-analysis of randomized controlled trials
- PMID: 35119026
- PMCID: PMC8812607
- DOI: 10.1097/MD.0000000000028742
Programmed intermittent epidural bolus in parturients: A meta-analysis of randomized controlled trials
Abstract
Background: To evaluate the efficacy and safety of programmed intermittent epidural bolus (PIEB) in parturients.
Methods: The PubMed, Embase, and the Cochrane Library (from inception to July 2021) were searched for identification of randomized placebo-controlled trials in which PIEB was applied in parturients. The outcomes were the effect of analgesia, satisfaction score, mode of delivery, duration of labor, neonatal condition, and adverse events. The pooled odds ratios (OR), weighted mean difference (WMD), and 95% confidence intervals (CIs) were calculated using random- and fixed-effects models.
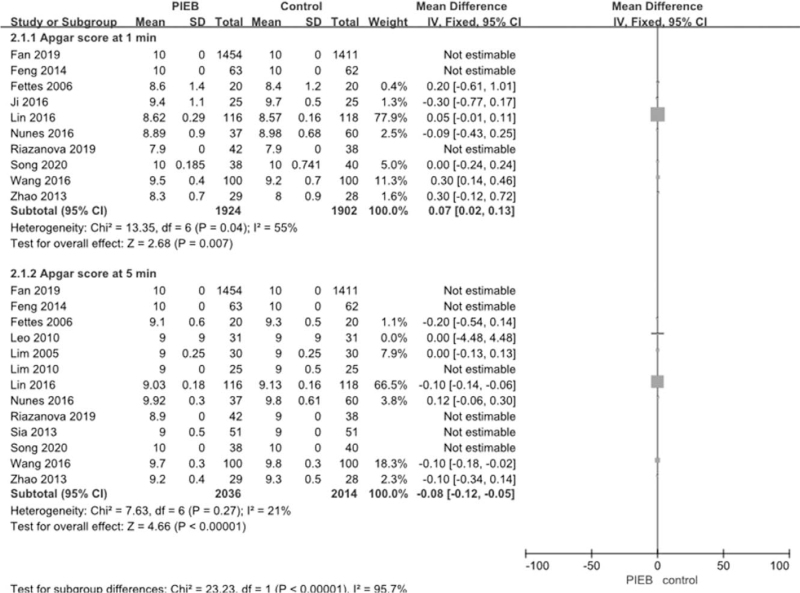
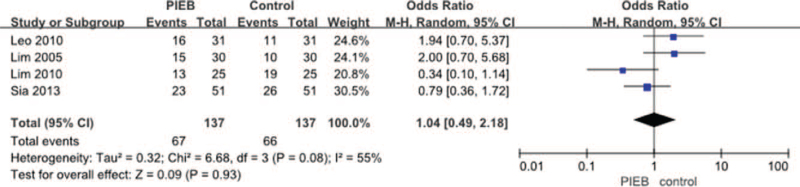
Results: PIEB was found to be associated with decreased total consumption of ropivacaine (WMD = -15.83, 95% CI: -19.06 to -12.60, P < .00001; I2 = 61%; P for heterogeneity = .04), total consumption of sufentanil (WMD = -4.93, 95% CI: -6.87 to 2.98, P < .00001; I2 = 68%; P for heterogeneity = .05), numbers of patients who require patient-controlled epidural analgesia bolus (OR = 0.27, 95% CI: 0.14-0.51, P < .0001; I2 = 65%; P for heterogeneity = .01), the number of attempts (WMD = -4.12, 95% CI: -7.21 to -1.04, P = .009; I2 = 100%; P for heterogeneity < .00001), rate of breakthrough pain (OR = 0.47, 95% CI: 0.28-0.80, P = .005; I2 = 47%; P for heterogeneity = .09). Eight studies focus on the duration of analgesia. After by meta-analysis, we found that the pain visual analogue scale (VAS) score at 30 minutes, 2 hours, 4 hours, and 5 hours in PIEB group was significantly lower when compared with control group, (WMD = -0.15, 95% CI: -0.26 to -0.04, P = .006; I2 = 0%; P for heterogeneity = .64), (WMD = -0.79, 95% CI: -1.32 to 0.25, P = .004; I2 = 97%; P for heterogeneity < .00001), (WMD = -1.00, 95% CI: -1.08 to -0.91, P < .00001; I2 = 0%; P for heterogeneity = .67), (WMD = -1.81, 95% CI: -3.23 to -0.39, P = .01; I2 = 98%; P for heterogeneity < .00001), respectively. Nineteen studies discussed the mode of delivery between 2 groups. The results suggest that the rate of normal delivery is significantly higher in PIEB group compared with control group (OR = 1.37, 95% CI: 1.08-1.75, P = .01). The time of first and second stage of labor are significantly shorter in PIEB group compared with control group, the result is (WMD = -10.52, 95% CI: -14.74 to 4.76, P < .00001; I2 = 0%; P for heterogeneity = .86), (WMD = -1.48, 95% CI: -2.26 to -0.69, P = .0002; I2 = 35%; P for heterogeneity = .10), respectively. Thirteen studies concerned the satisfaction score of patients. The satisfaction score of patients in the PIEB group was significantly higher when compared with control group (WMD = 0.91, 95% CI: 0.42-1.39, P = .0003; I2 = 98%; P for heterogeneity < .00001). The Apgar score at 1, 5 minutes in PIEB group are significantly higher (WMD = 0.07, 95% CI: 0.02-0.13 P = .007; I2 = 55%; P for heterogeneity = .04), (WMD = -0.08, 95% CI: -0.12 to -0.05, P < .00001; I2 = 21%; P for heterogeneity = .27), respectively.
Conclusions: PIEB is a good alternative for labor analgesia with better analgesic effect, maternal and infant outcome.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures


















References
-
- Song YJ, Du WJ, Zhou SQ, et al. Effect of dural puncture epidural technique combined with programmed intermittent epidural bolus on labor analgesia onset and maintenance: a randomized controlled trial. Anesth Analg 2021;132:971–8. - PubMed
-
- Wang LY, Wu ZH, Hu LJ, et al. Programmed intermittent epidural bolus for post-cesarean delivery analgesia: a randomized controlled double-blind trial. J Anesth 2021;doi: 10.1007/s00540-021-03002-x. - PubMed
-
- Gaiser RR, Lewin SB, Cheek TG, et al. Effects of immediately initiating an epidural infusion in the combined spinal and epidural technique in nulliparous parturients. Reg Anesth Pain Med 2000;25:223–7. - PubMed
-
- Chua SM, Sia AT. Automated intermittent epidural boluses improve analgesia induced by intrathecal fentanyl during labour. Can J Anaesth 2004;51:581–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
