

Culprit Medications and Risk Factors Associated with Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Population-Based Nested Case-Control Study
- PMID: 35119606
- PMCID: PMC8814784
- DOI: 10.1007/s40257-021-00661-0
Culprit Medications and Risk Factors Associated with Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Population-Based Nested Case-Control Study
Abstract
Objective: Our objective was to describe the incidence of Stevens-Johnson syndrome/toxic epidermal necrolysis (SJS/TEN) in a large unselected cohort, to validate the culprit drugs involved and the frequency of SJS/TEN for each drug, and to analyze the clinical risk factors for SJS/TEN.
Methods: Using the computerized database of Clalit Health Services, we identified all adult patients with a new SJS/TEN diagnosis between 1 January, 2008 and 30 June, 2019 and validated each case. Cumulative incidence of SJS/TEN for each culprit drug was calculated by dividing the number of valid cases by the total number of new users of the drug in the study period. Using risk-set sampling, 20 controls were matched to each case by sex and age on the index date for a nested case-control analysis. Multivariable conditional logistic regression was used to estimate the odds ratio and 95% confidence interval for the association of incident SJS/TEN with chronic diseases.
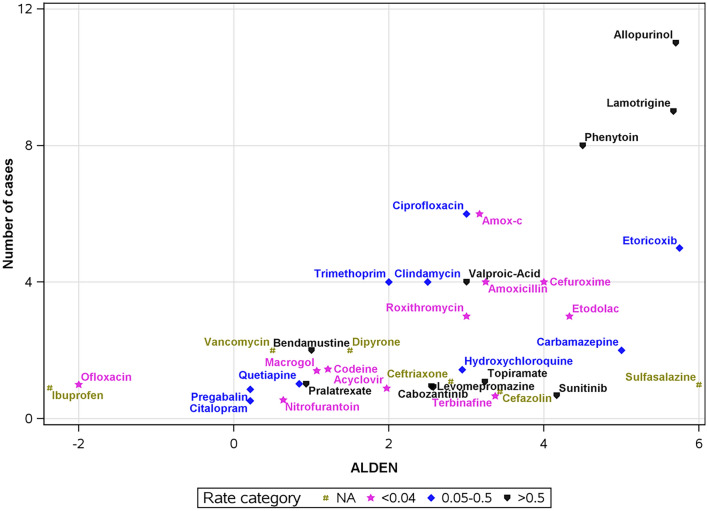
Results: We identified 87 adult cases of true/probable SJS/TEN between 1 January, 2008 and 30 June, 2019. Culprit drugs [with ALDEN scores ascertained as at least probable (≥ 4)] associated with the highest absolute risks were phenytoin, lamotrigine, and allopurinol with 3.56, 2.82, and 1.10 SJS/TEN cases/10,000 new users, respectively. Additional drugs with mean ALDEN scores ≥ 4 were sunitinib, sulfasalazine, carbamazepine, etoricoxib, etodolac, and cefuroxime, cumulative incidence: 13.57, 0.72, 0.32, 0.05, 0.02, and 0.02/10,000 new users, respectively. Previous diagnosis of systemic lupus erythematosus, psoriasis, previous drug allergies, epilepsy, malignancy, history of cerebrovascular accident, and history of diabetes mellitus were associated with an increased risk for SJS/TEN, odds ratios (95% confidence interval):17.41 (1.31-230.72), 10.28 (3.61-29.31), 5.21 (2.95-9.19), 4.92 (1.88-12.85), 3.17 (1.77-5.66), 2.61 (1.26-5.41), and 1.98 (1.12-3.53), respectively.
Conclusions: Attention should be drawn to drugs assessed by high ALDEN scores that were associated with high absolute risks for SJS/TEN. Psoriasis, former drug allergies, in addition to systemic lupus erythematosus, malignancy, history of cerebrovascular accident, and diabetes mellitus were associated with increased SJS/TEN risk in our analysis.
© 2022. The Author(s), under exclusive licence to Springer Nature Switzerland AG.
Conflict of interest statement
No conflict of interest reported for all authors.
Figures
References
-
- Mockenhaupt M, Viboud C, Dunant A, Naldi L, Halevy S, Bouwes Bavinck JN, et al. Stevens–Johnson syndrome and toxic epidermal necrolysis: assessment of medication risks with emphasis on recently marketed drugs. The EuroSCAR-study. J Invest Dermatol. 2008;128(1):35–44. doi: 10.1038/sj.jid.5701033. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
