

Sex Differences in Risk of Severe Adverse Events in Patients Receiving Immunotherapy, Targeted Therapy, or Chemotherapy in Cancer Clinical Trials
- PMID: 35119908
- PMCID: PMC9061143
- DOI: 10.1200/JCO.21.02377
Sex Differences in Risk of Severe Adverse Events in Patients Receiving Immunotherapy, Targeted Therapy, or Chemotherapy in Cancer Clinical Trials
Abstract
Purpose: Women have more adverse events (AEs) from chemotherapy than men, but few studies have investigated sex differences in immune or targeted therapies. We examined AEs by sex across different treatment domains.
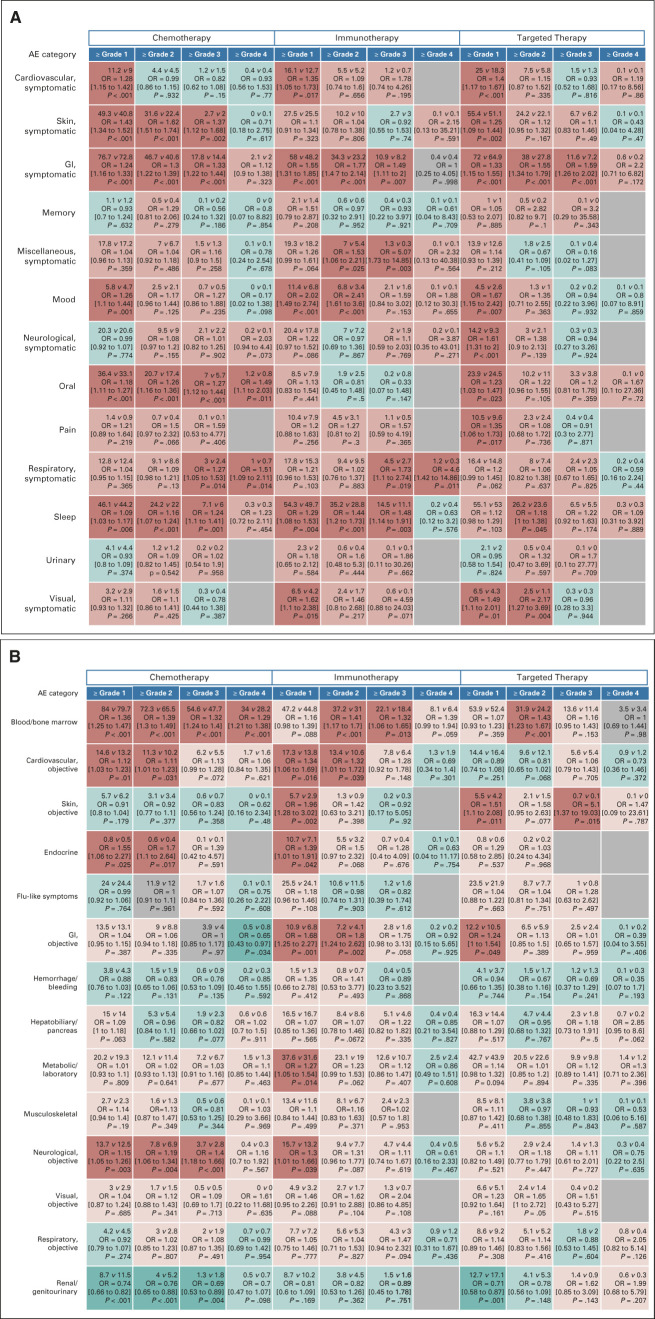
Methods: We analyzed treatment-related AEs by sex in SWOG phase II and III clinical trials conducted between 1980 and 2019, excluding sex-specific cancers. AE codes and grade were categorized using the Common Terminology Criteria for Adverse Events. Symptomatic AEs were defined as those aligned with the National Cancer Institute's Patient-Reported Outcome-Common Terminology Criteria for Adverse Events; laboratory-based or observable/measurable AEs were designated as objective (hematologic v nonhematologic). Multivariable logistic regression was used, adjusting for age, race, and disease prognosis. Thirteen symptomatic and 14 objective AE categories were examined.
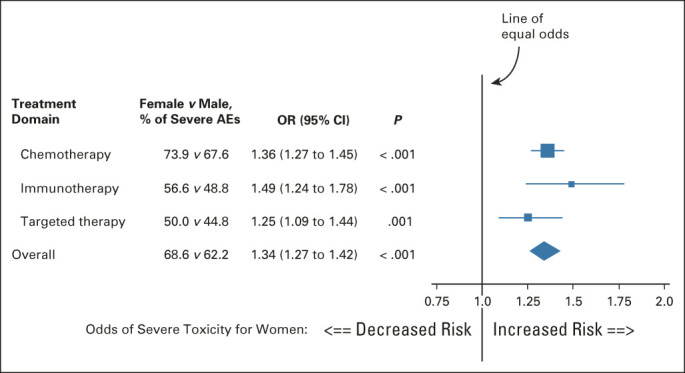
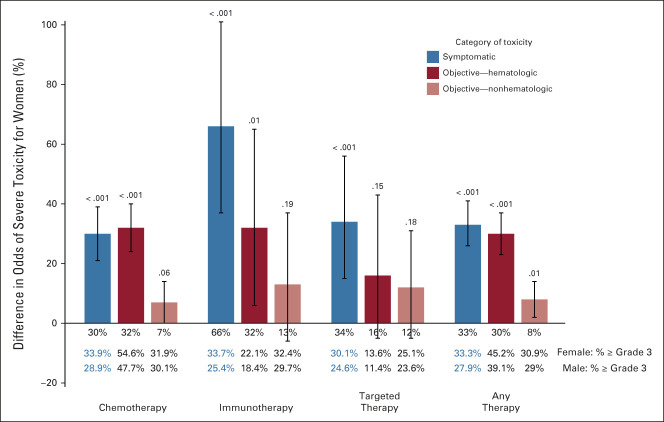
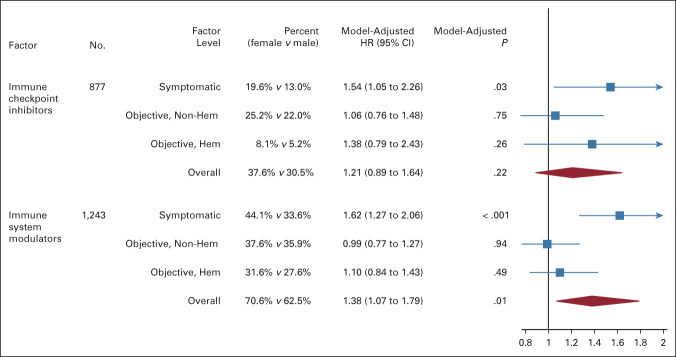
Results: In total, N = 23,296 patients (women, 8,838 [37.9%]; men, 14,458 [62.1%]) from 202 trials experiencing 274,688 AEs were analyzed; 17,417 received chemotherapy, 2,319 received immunotherapy, and 3,560 received targeted therapy. Overall, 64.6% (n = 15,051) experienced one or more severe (grade ≥ 3) AEs. Women had a 34% increased risk of severe AEs compared with men (odds ratio [OR] = 1.34; 95% CI, 1.27 to 1.42; P < .001), including a 49% increased risk among those receiving immunotherapy (OR = 1.49; 95% CI, 1.24 to 1.78; P < .001). Women experienced an increased risk of severe symptomatic AEs among all treatments, especially immunotherapy (OR = 1.66; 95% CI, 1.37 to 2.01; P < .001). Women receiving chemotherapy or immunotherapy experienced increased severe hematologic AE. No statistically significant sex differences in risk of nonhematologic AEs were found.
Conclusion: The greater severity of both symptomatic AEs and hematologic AEs in women across multiple treatment modalities indicates that broad-based sex differences exist. This could be due to differences in AE reported, pharmacogenomics of drug metabolism/disposition, total dose received, and/or adherence to therapy. Particularly large sex differences were observed for patients receiving immunotherapy, suggesting that studying AEs from these agents is a priority.
Conflict of interest statement
Figures
Comment in
-
Sex differences in serious adverse drug reactions in patients receiving immunotherapy, targeted therapy, or chemotherapy: a disproportionality analysis of the VigiBase®.Eur J Clin Pharmacol. 2022 Aug;78(8):1355-1356. doi: 10.1007/s00228-022-03332-z. Epub 2022 May 13. Eur J Clin Pharmacol. 2022. PMID: 35562621 No abstract available.
Similar articles
-
Adverse event profile for immunotherapy agents compared with chemotherapy in solid organ tumors: a systematic review and meta-analysis of randomized clinical trials.Ann Oncol. 2020 Jan;31(1):50-60. doi: 10.1016/j.annonc.2019.10.008. Ann Oncol. 2020. PMID: 31912796
-
Assessment of Adverse Events From the Patient Perspective in a Phase 3 Metastatic Castration-Resistant Prostate Cancer Clinical Trial.JAMA Oncol. 2020 Feb 1;6(2):e193332. doi: 10.1001/jamaoncol.2019.3332. Epub 2020 Feb 13. JAMA Oncol. 2020. PMID: 31556911 Free PMC article. Clinical Trial.
-
Feasibility Assessment of Patient Reporting of Symptomatic Adverse Events in Multicenter Cancer Clinical Trials.JAMA Oncol. 2017 Aug 1;3(8):1043-1050. doi: 10.1001/jamaoncol.2016.6749. JAMA Oncol. 2017. PMID: 28208174 Free PMC article. Clinical Trial.
-
Cutaneous side effects and types of dermatological reactions in metastatic melanoma patients treated by immunotherapies or targeted therapies: A retrospective single center study.Dermatol Ther. 2022 Jun;35(6):e15492. doi: 10.1111/dth.15492. Epub 2022 May 10. Dermatol Ther. 2022. PMID: 35384181 Free PMC article.
-
Natalizumab for induction of remission in Crohn's disease.Cochrane Database Syst Rev. 2018 Aug 1;8(8):CD006097. doi: 10.1002/14651858.CD006097.pub3. Cochrane Database Syst Rev. 2018. PMID: 30068022 Free PMC article.
Cited by
-
Sex as a Biological Variable in Early-Phase Oncology Clinical Trials: Enhancing the Path to Personalised Medicine.Heliyon. 2024 Jun 7;10(12):e32597. doi: 10.1016/j.heliyon.2024.e32597. eCollection 2024 Jun 30. Heliyon. 2024. PMID: 39183838 Free PMC article. Review.
-
Sex-biased gene expression and gene-regulatory networks of sex-biased adverse event drug targets and drug metabolism genes.BMC Pharmacol Toxicol. 2024 Jan 2;25(1):5. doi: 10.1186/s40360-023-00727-1. BMC Pharmacol Toxicol. 2024. PMID: 38167211 Free PMC article.
-
Toxicity, disease management and outcome of treatment with immune checkpoint inhibitors by sex in patients with cancer and preexisting autoimmune disease.Oncol Lett. 2023 Jul 18;26(3):377. doi: 10.3892/ol.2023.13963. eCollection 2023 Sep. Oncol Lett. 2023. PMID: 37559593 Free PMC article.
-
Impact of sex differences on patients with neuroendocrine neoplasms during hospital admission.Ther Adv Med Oncol. 2024 Dec 15;16:17588359241292271. doi: 10.1177/17588359241292271. eCollection 2024. Ther Adv Med Oncol. 2024. PMID: 39687054 Free PMC article.
-
Cognitive Symptoms Across Diverse Cancers.JAMA Netw Open. 2024 Aug 1;7(8):e2430833. doi: 10.1001/jamanetworkopen.2024.30833. JAMA Netw Open. 2024. PMID: 39196555 Free PMC article.
References
-
- Legato MJ, Johnson PA, Manson JE: Consideration of sex differences in medicine to improve Health care and patient outcomes. JAMA 316:1865-1866, 2016 - PubMed
-
- Özdemir BC, Csajka C, Dotto GP, et al. : Sex differences in efficacy and toxicity of systemic treatments: An undervalued issue in the era of precision Oncology. J Clin Oncol 36:2680-2683, 2018 - PubMed
-
- Chansky K, Benedetti J, Macdonald JS: Differences in toxicity between men and women treated with 5-fluorouracil therapy for colorectal carcinoma. Cancer 103:1165-1171, 2005 - PubMed
-
- Gotay CC, Phillips PH, Cheson BD: Male-female differences in the impact of cancer therapy. Oncology (Williston Park) 7:67-74, 1993. discussion 74, 77 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
