Association of ischemic stroke onset time with presenting severity, acute progression, and long-term outcome: A cohort study
- PMID: 35120123
- PMCID: PMC8815976
- DOI: 10.1371/journal.pmed.1003910
Association of ischemic stroke onset time with presenting severity, acute progression, and long-term outcome: A cohort study
Abstract
Background: Preclinical data suggest circadian variation in ischemic stroke progression, with more active cell death and infarct growth in rodent models with inactive phase (daytime) than active phase (nighttime) stroke onset. We aimed to examine the association of stroke onset time with presenting severity, early neurological deterioration (END), and long-term functional outcome in human ischemic stroke.
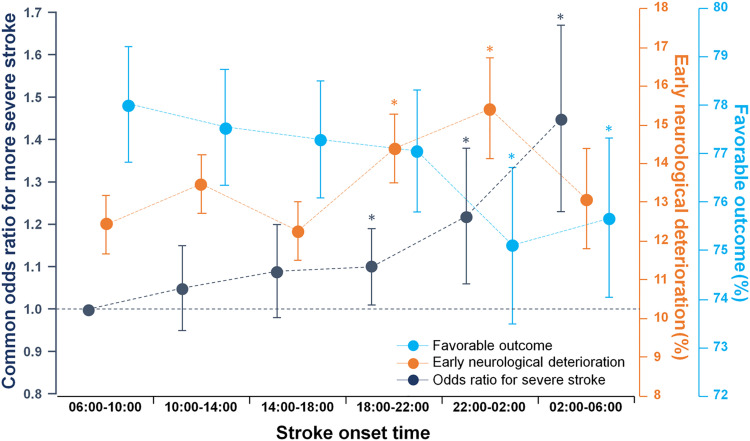
Methods and findings: In a Korean nationwide multicenter observational cohort study from May 2011 to July 2020, we assessed circadian effects on initial stroke severity (National Institutes of Health Stroke Scale [NIHSS] score at admission), END, and favorable functional outcome (3-month modified Rankin Scale [mRS] score 0 to 2 versus 3 to 6). We included 17,461 consecutive patients with witnessed ischemic stroke within 6 hours of onset. Stroke onset time was divided into 2 groups (day-onset [06:00 to 18:00] versus night-onset [18:00 to 06:00]) and into 6 groups by 4-hour intervals. We used mixed-effects ordered or logistic regression models while accounting for clustering by hospitals. Mean age was 66.9 (SD 13.4) years, and 6,900 (39.5%) were women. END occurred in 2,219 (12.7%) patients. After adjusting for covariates including age, sex, previous stroke, prestroke mRS score, admission NIHSS score, hypertension, diabetes, hyperlipidemia, smoking, atrial fibrillation, prestroke antiplatelet use, prestroke statin use, revascularization, season of stroke onset, and time from onset to hospital arrival, night-onset stroke was more prone to END (adjusted incidence 14.4% versus 12.8%, p = 0.006) and had a lower likelihood of favorable outcome (adjusted odds ratio, 0.88 [95% CI, 0.79 to 0.98]; p = 0.03) compared with day-onset stroke. When stroke onset times were grouped by 4-hour intervals, a monotonic gradient in presenting NIHSS score was noted, rising from a nadir in 06:00 to 10:00 to a peak in 02:00 to 06:00. The 18:00 to 22:00 and 22:00 to 02:00 onset stroke patients were more likely to experience END than the 06:00 to 10:00 onset stroke patients. At 3 months, there was a monotonic gradient in the rate of favorable functional outcome, falling from a peak at 06:00 to 10:00 to a nadir at 22:00 to 02:00. Study limitations include the lack of information on sleep disorders and patient work/activity schedules.
Conclusions: Night-onset strokes, compared with day-onset strokes, are associated with higher presenting neurologic severity, more frequent END, and worse 3-month functional outcome. These findings suggest that circadian time of onset is an important additional variable for inclusion in epidemiologic natural history studies and in treatment trials of neuroprotective and reperfusion agents for acute ischemic stroke.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: For the following roles, Dr. JS receives contracted hourly payments: Abbott / St. Jude Medical Clinical Trial Steering Committee Medtronic Clinical Trial Steering Committee BrainsGate Clinical Trial Steering Committee Stryker Clinical Trial Steering Committee Boehringer-Ingelheim (Prevention Only) Clinical Trial Steering Committee Cerenovus / Neuravi) Clinical Trial Steering Committee Phagenesis Clinical Trial Steering Committee For the following role, Dr. JS receives contracted stock options: Rapid Medical Clinical Trial Steering Committee.
Figures