

Color-coded summation images for the evaluation of blood flow in endovascular aortic dissection fenestration
- PMID: 35120493
- PMCID: PMC8817583
- DOI: 10.1186/s12880-022-00744-2
Color-coded summation images for the evaluation of blood flow in endovascular aortic dissection fenestration
Abstract
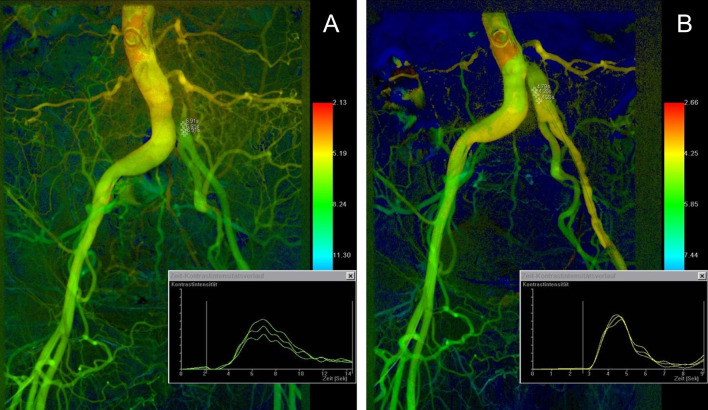
Background: To analyze the benefit of color-coded summation images in the assessment of target lumen perfusion in patients with aortic dissection and malperfusion syndrome before and after fluoroscopy-guided aortic fenestration.
Methods: Between December 2011 and April 2020 25 patients with Stanford type A (n = 13) or type B dissection (n = 12) and malperfusion syndromes were treated with fluoroscopy-guided fenestration of the dissection flap using a re-entry catheter. The procedure was technically successful in 100% of the cases and included additional iliofemoral stent implantation in four patients. Intraprocedural systolic blood pressure measurements for gradient evaluation were performed in 19 cases. Post-processed color-coded DSA images were obtained from all DSA series before and following fenestration. Differences in time to peak (dTTP) values in the compromised aortic lumen and transluminal systolic blood pressure gradients were analyzed retrospectively. Correlation analysis between dTTP and changes in blood pressure gradients was performed.
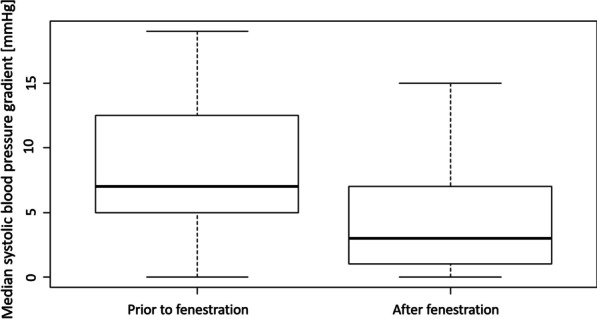
Results: Mean TTP prior to dissection flap fenestration was 6.85 ± 1.35 s. After fenestration, mean TTP decreased significantly to 4.96 ± 0.94 s (p < 0.001). Available systolic blood pressure gradients between the true and the false lumen were reduced by a median of 4.0 mmHg following fenestration (p = 0.031), with significant reductions in Stanford type B dissections (p = 0.013) and minor reductions in type A dissections (p = 0.530). A moderate correlation with no statistical significance was found between dTTP and the difference in systolic blood pressure (r = 0.226; p = 0.351).
Conclusions: Hemodynamic parameters obtained from color-coded DSA confirmed a significant reduction of TTP values in the aortic target lumen in terms of an improved perfusion in the compromised aortic region. Color-coded DSA might thus be a suitable complementary tool in the assessment of complex vascular patterns prevailing in aortic dissections, especially when blood pressure measurements are not conclusive or feasible.
Keywords: Angiography; Aortic dissection; Color-coding; DSA; Endovascular; Fenestration.
© 2022. The Author(s).
Conflict of interest statement
T.E. is an employee of Siemens Healthineers. The other authors declare that they have no competing interests.
Figures


References
-
- Suzuki T, Mehta RH, Ince H, et al. Clinical profiles and outcomes of acute type B aortic dissection in the current era: lessons from the International Registry of Aortic Dissection (IRAD) Circulation. 2003;108(Suppl 1):II312–II317. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
