

Genomic characterization of metastatic patterns from prospective clinical sequencing of 25,000 patients
- PMID: 35120664
- PMCID: PMC9147702
- DOI: 10.1016/j.cell.2022.01.003
Genomic characterization of metastatic patterns from prospective clinical sequencing of 25,000 patients
Abstract
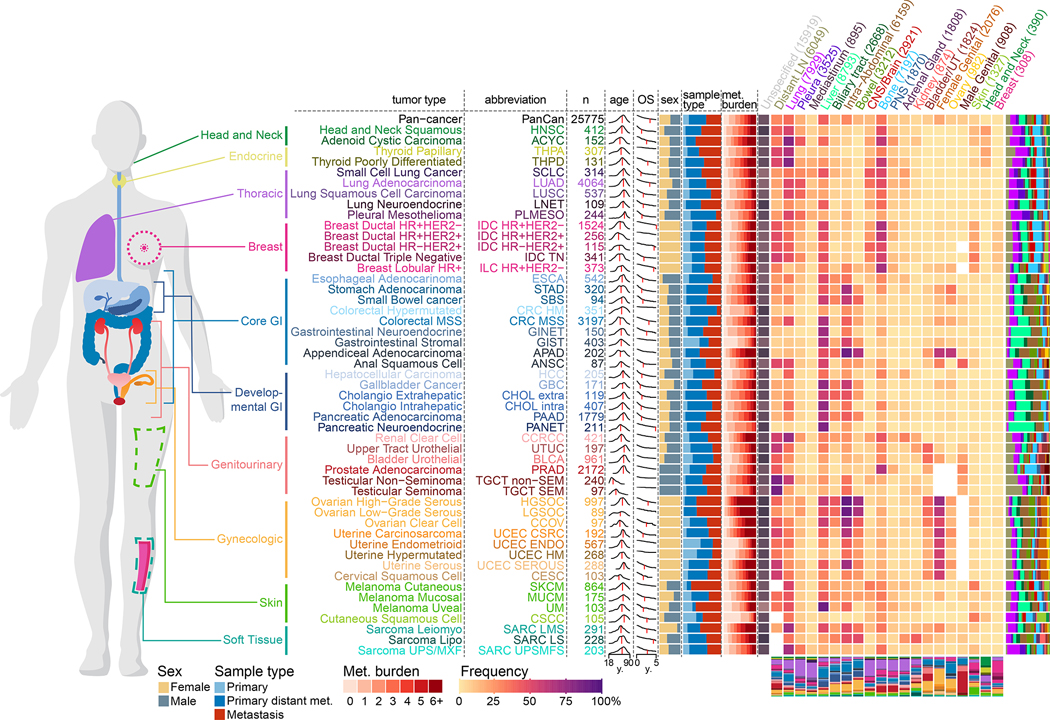
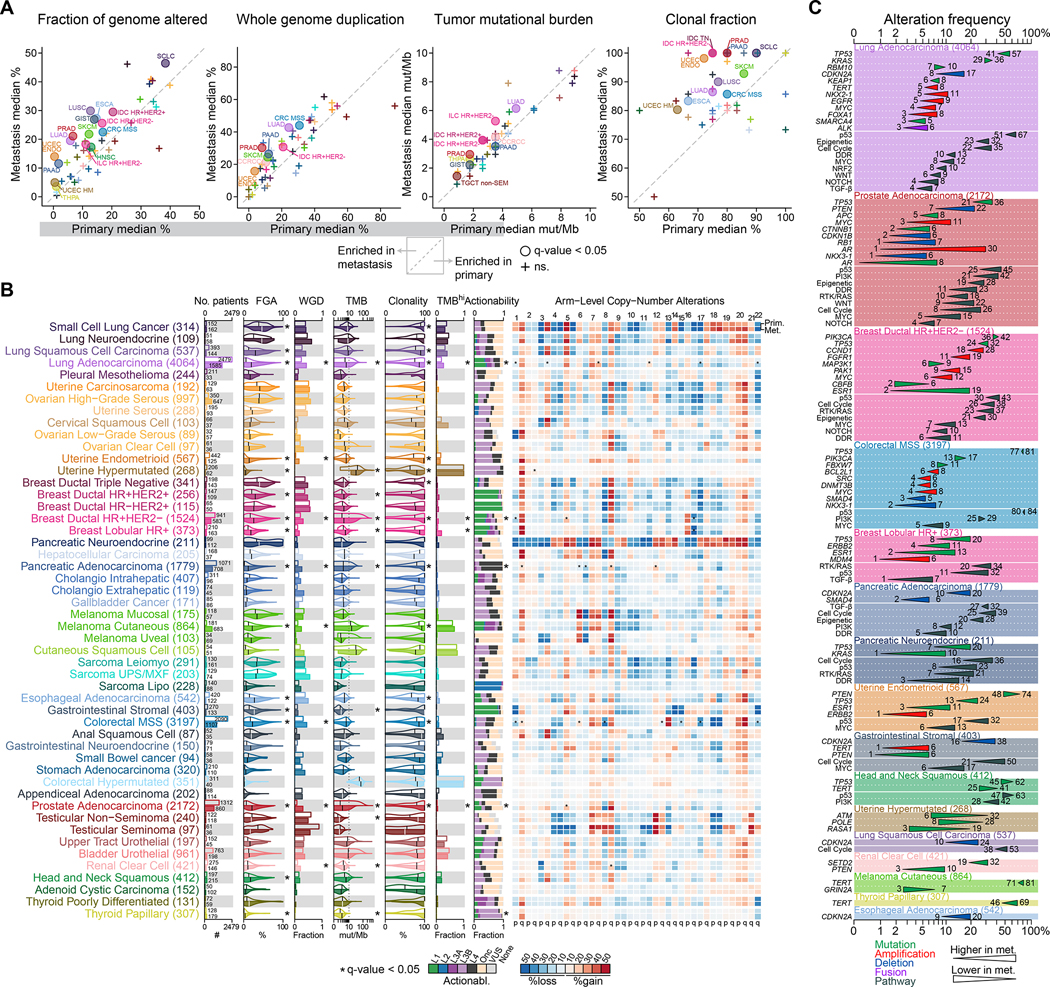
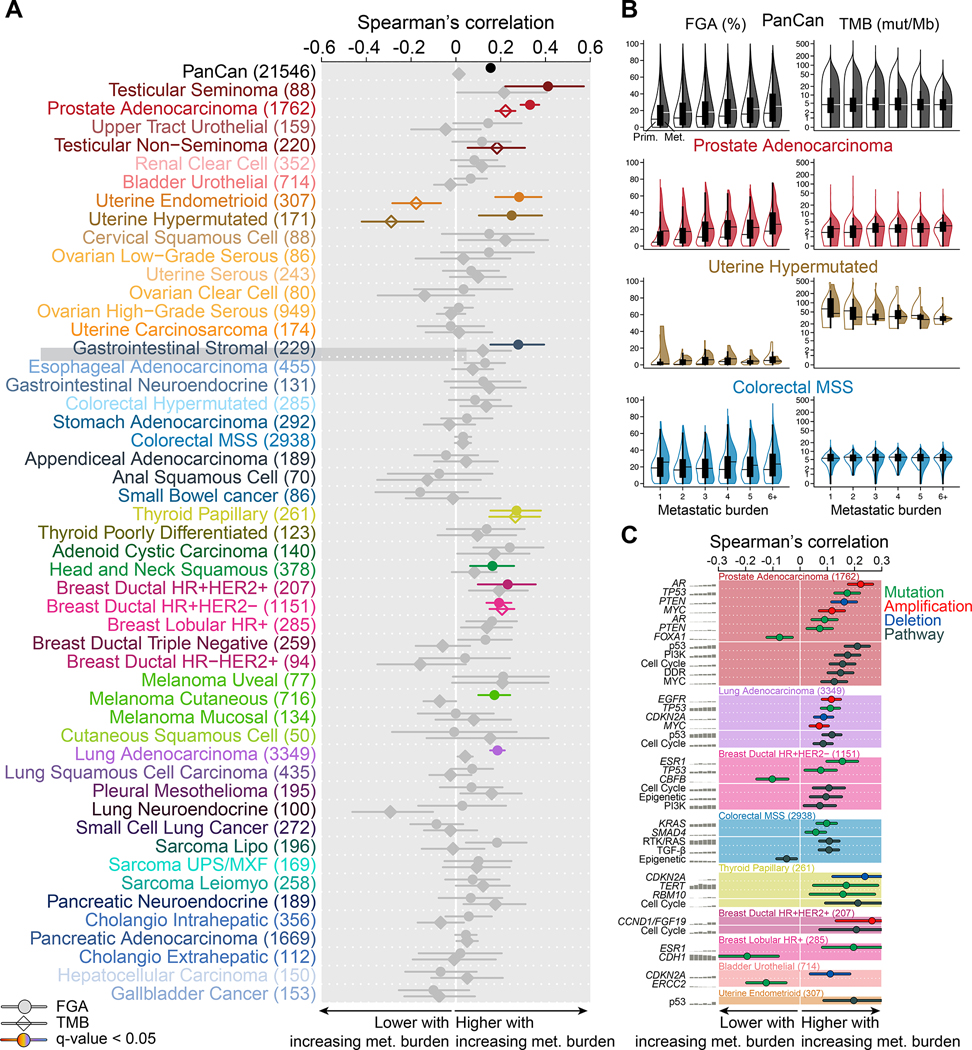
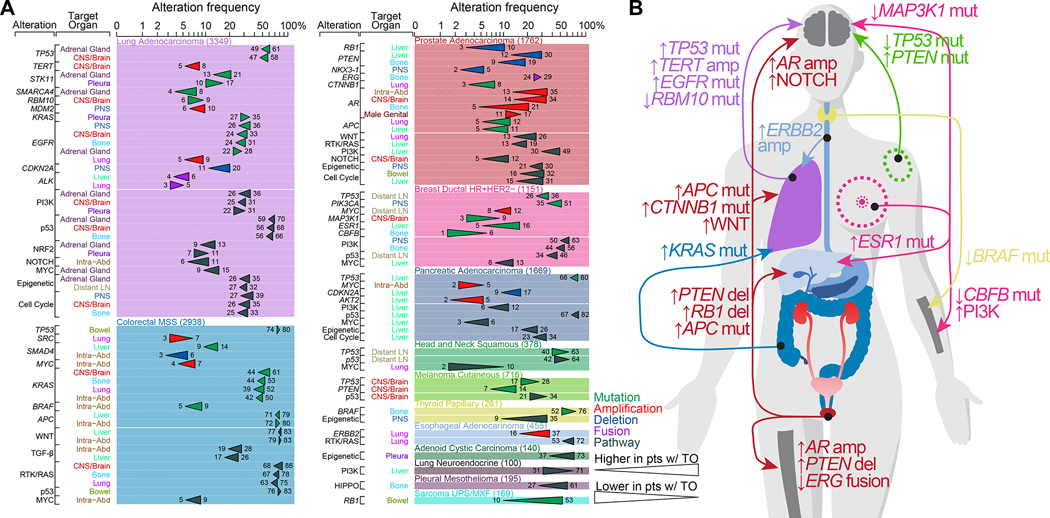
Metastatic progression is the main cause of death in cancer patients, whereas the underlying genomic mechanisms driving metastasis remain largely unknown. Here, we assembled MSK-MET, a pan-cancer cohort of over 25,000 patients with metastatic diseases. By analyzing genomic and clinical data from this cohort, we identified associations between genomic alterations and patterns of metastatic dissemination across 50 tumor types. We found that chromosomal instability is strongly correlated with metastatic burden in some tumor types, including prostate adenocarcinoma, lung adenocarcinoma, and HR+/HER2+ breast ductal carcinoma, but not in others, including colorectal cancer and high-grade serous ovarian cancer, where copy-number alteration patterns may be established early in tumor development. We also identified somatic alterations associated with metastatic burden and specific target organs. Our data offer a valuable resource for the investigation of the biological basis for metastatic spread and highlight the complex role of chromosomal instability in cancer progression.
Keywords: DNA sequencing; cancer; clinical sequencing; genomics; metastasis; molecular profiling; mutations; next-generation sequencing; organotropism; pan-cancer.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests S.C. receives consulting fees from Novartis, Lilly, and Sanofi and research funding from Daiichi-Sankyo and Paige.ai. J.J.H. receives consulting fees from Bristol Myers Squibb, Merck, Exelexis, Eisai, QED, Cytomx, Zymeworks, Adaptiimmune, and ImVax and research funding from Bristol Myers Squibb. C.A.I.-D. receives research funding from Bristol Myers Squibb. P. Razavi received consultation/Ad board/Honoraria from Novartis, Foundation Medicine, AstraZeneca, Epic Sciences, Inivata, Natera, and Tempus and institutional grant/funding from Grail, Illumina, Novartis, Epic Sciences, and ArcherDx. C.M.R. has consulted regarding oncology drug development with AbbVie, Amgen, Astra Zeneca, Epizyme, Genentech/Roche, Ipsen, Jazz, Lilly, and Syros and serves on the scientific advisory boards of Bridge Medicines, Earli, and Harpoon Therapeutics. D.Z. receives research funding from Astra Zeneca, Plexxikon, and Genentech and consulting fees from Merck, Synlogic Therapeutics, GSK, Bristol Myers Squibb, Genentech, Xencor, Memgen, Immunos, Agenus, Hookipa, Calidi, and Synthekine. B.W. has an ad hoc membership advisory board Repare Therapeutics. W.A. receives speaking honoraria from Roche, Medscape, Aptitude Health, and Clinical Education Alliance; consulting fees from Clovis Oncology, Janssen, ORIC pharmaceuticals, Daiichi Sankyo; and research funding from AstraZeneca, Zenith Epigenetics, Clovis Oncology, ORIC pharmaceuticals, and Epizyme. G.K.A.-A. receives research funding from Arcus, Agios, Astra Zeneca, Bayer, BioNtech, BMS, Celgene, Flatiron, Genentech/Roche, Genoscience, Incyte, Polaris, Puma, QED, Sillajen, and Yiviva and consulting fees from Adicet, Agios, Astra Zeneca, Alnylam, Autem, Bayer, Beigene, Berry Genomics, Cend, Celgene, CytomX, Eisai, Eli Lilly, Exelixis, Flatiron, Genentech/Roche, Genoscience, Helio, Incyte, Ipsen, Legend Biotech, Loxo, Merck, MINA, Nerviano, QED, Redhill, Rafael, Silenseed, Sillajen, Sobi, Surface Oncology, Therabionics, Twoxar, Vector, and Yiviva. E.M.O. receives research funding from Genentech/Roche, Celgene/BMS, BioNTech, BioAtla, AstraZeneca, Arcus, Elicio, Parker Institute, and AstraZeneca and consulting fees from Cytomx Therapeutics (DSMB), Rafael Therapeutics (DSMB), Sobi, Silenseed, Tyme, Seagen, Molecular Templates, Boehringer Ingelheim, BioNTech, Ipsen, Polaris, Merck, IDEAYA, Cend, AstraZeneca, Noxxon, BioSapien, Bayer (spouse), Genentech-Roche (spouse), Celgene-BMS (spouse), and Eisai (spouse). M.A.P. receive consulting fees from BMS, Merck, Array BioPharma, Novartis, Incyte, NewLink Genetics, Aduro, Eisai, and Pfizer; honoraria from BMS and Merck; research support from RGenix, Infinity, BMS, Merck, Array BioPharma, Novartis, and AstraZeneca. G.J.R. has institutional research funding from Mirait, Takeda, Merck, Roche, Novartis, and Pfizer. S.F.B. holds a patent related to some of the work described targeting CIN in advanced cancer. He owns equity in, receives compensation from, and serves as a consultant and the scientific advisory board and board of directors of Volastra Therapeutics Inc. A.N.S. has advisory board/personal fees from Bristol-Myers Squibb, Immunocore, and Castle Biosciences; research support from Bristol-Myers Squibb, Immunocore, Xcovery, Polaris, Novartis, Pfizer, and Checkmate Pharmaceuticals; and research funding from OBI-Pharma, GSK, Silenseed, BMS, and Lilly. R.Y. receives consulting fees from Array BioPharma/Pfizer, Mirati Therapeutics, and Natera and research funding from Pfizer and Boehringer Ingelheim. D.R.J. is member of the advisory council for Astra Zeneca and member of the Clinical Trial Steering Committee for Merck. D.M. reports disclosures from AstraZeneca, Johnson & Johnson, Boston Scientific, Bristol-Myers Squibb, and Merck. S.P.S. is shareholder and consultant for Canexia Health Inc. M.F.B receives consulting fees from Roche, Eli Lilly, and PetDx and research funding from Grail. D.B.S. has received consulted for and received honoraria from Pfizer, Lilly/Loxo Oncology, Vividion Therapeutics, Scorpion Therapetuics, and BridgeBio. B.N. is an employee of Loxo Oncology at Lilly.
Figures
Comment in
-
Metastasis and organotropism: A look through the lens of large-scale clinical sequencing data.Cancer Cell. 2022 Feb 14;40(2):134-135. doi: 10.1016/j.ccell.2022.01.011. Epub 2022 Feb 3. Cancer Cell. 2022. PMID: 35120602
References
-
- Abida W, Armenia J, Gopalan A, Brennan R, Walsh M, Barron D, Danila D, Rathkopf D, Morris M, Slovin S, et al. (2017). Prospective Genomic Profiling of Prostate Cancer Across Disease States Reveals Germline and Somatic Alterations That May Affect Clinical Decision Making. JCO Precis Oncol 2017. - PMC - PubMed
-
- Ben-David U, and Amon A (2020). Context is everything: aneuploidy in cancer. Nat. Rev. Genet. 21, 44–62. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 CA252048/CA/NCI NIH HHS/United States
- DP5 OD026395/OD/NIH HHS/United States
- R01 CA245499/CA/NCI NIH HHS/United States
- R01 CA228216/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- R01 CA234361/CA/NCI NIH HHS/United States
- P50 CA221745/CA/NCI NIH HHS/United States
- P50 CA247749/CA/NCI NIH HHS/United States
- K08 CA230213/CA/NCI NIH HHS/United States
- P50 CA217694/CA/NCI NIH HHS/United States
- R01 CA256188/CA/NCI NIH HHS/United States
- P50 CA140146/CA/NCI NIH HHS/United States
- R37 CA266185/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
