

Integrating molecular profiles into clinical frameworks through the Molecular Oncology Almanac to prospectively guide precision oncology
- PMID: 35121878
- PMCID: PMC9082009
- DOI: 10.1038/s43018-021-00243-3
Integrating molecular profiles into clinical frameworks through the Molecular Oncology Almanac to prospectively guide precision oncology
Abstract
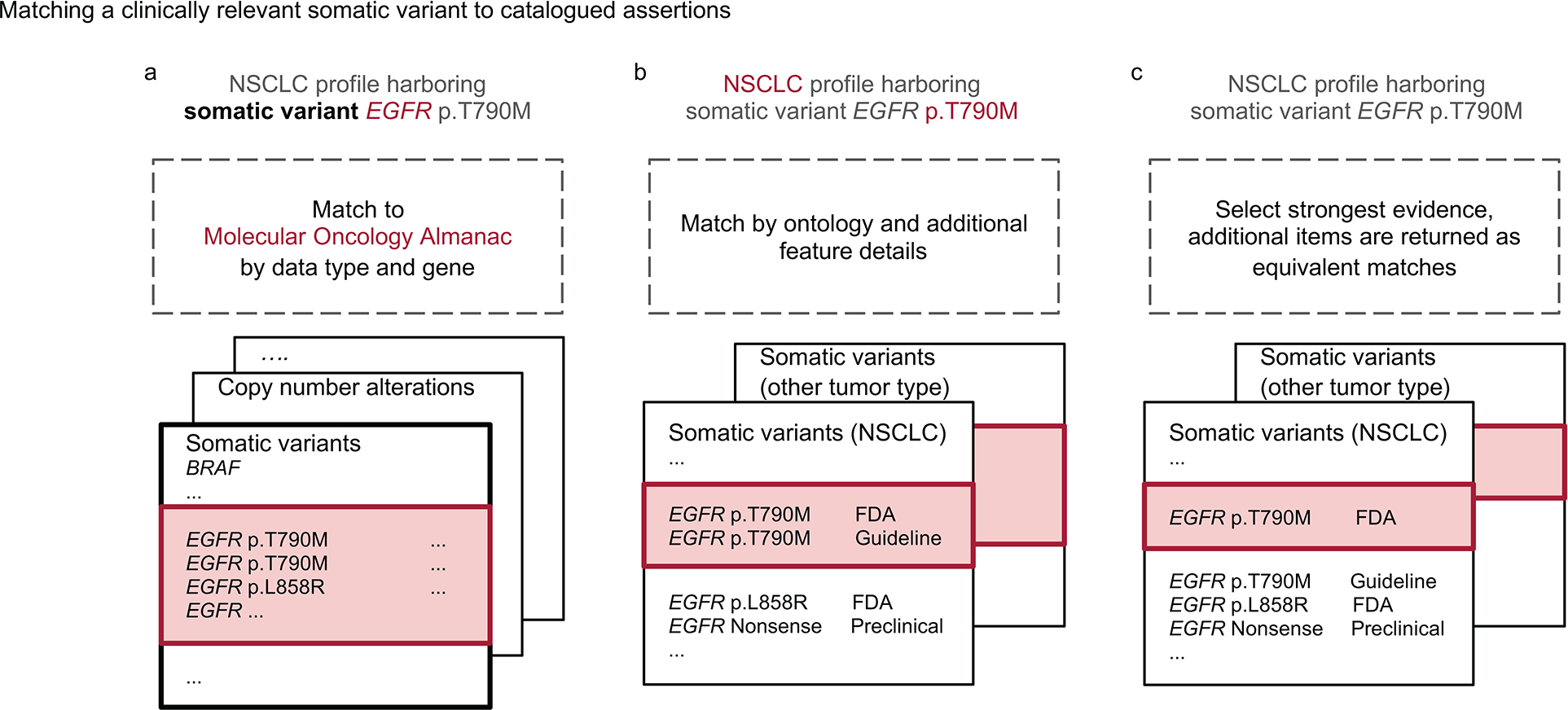
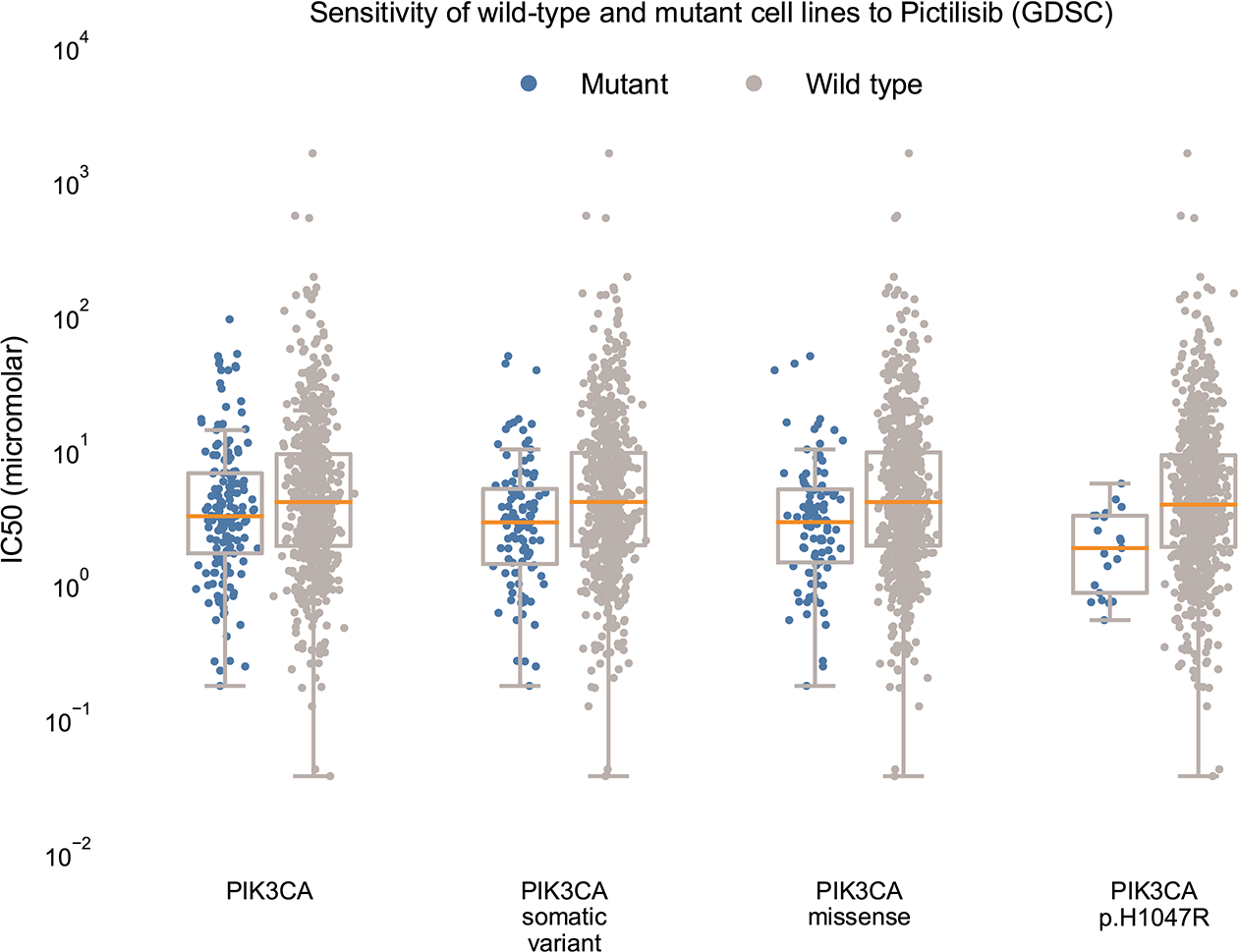
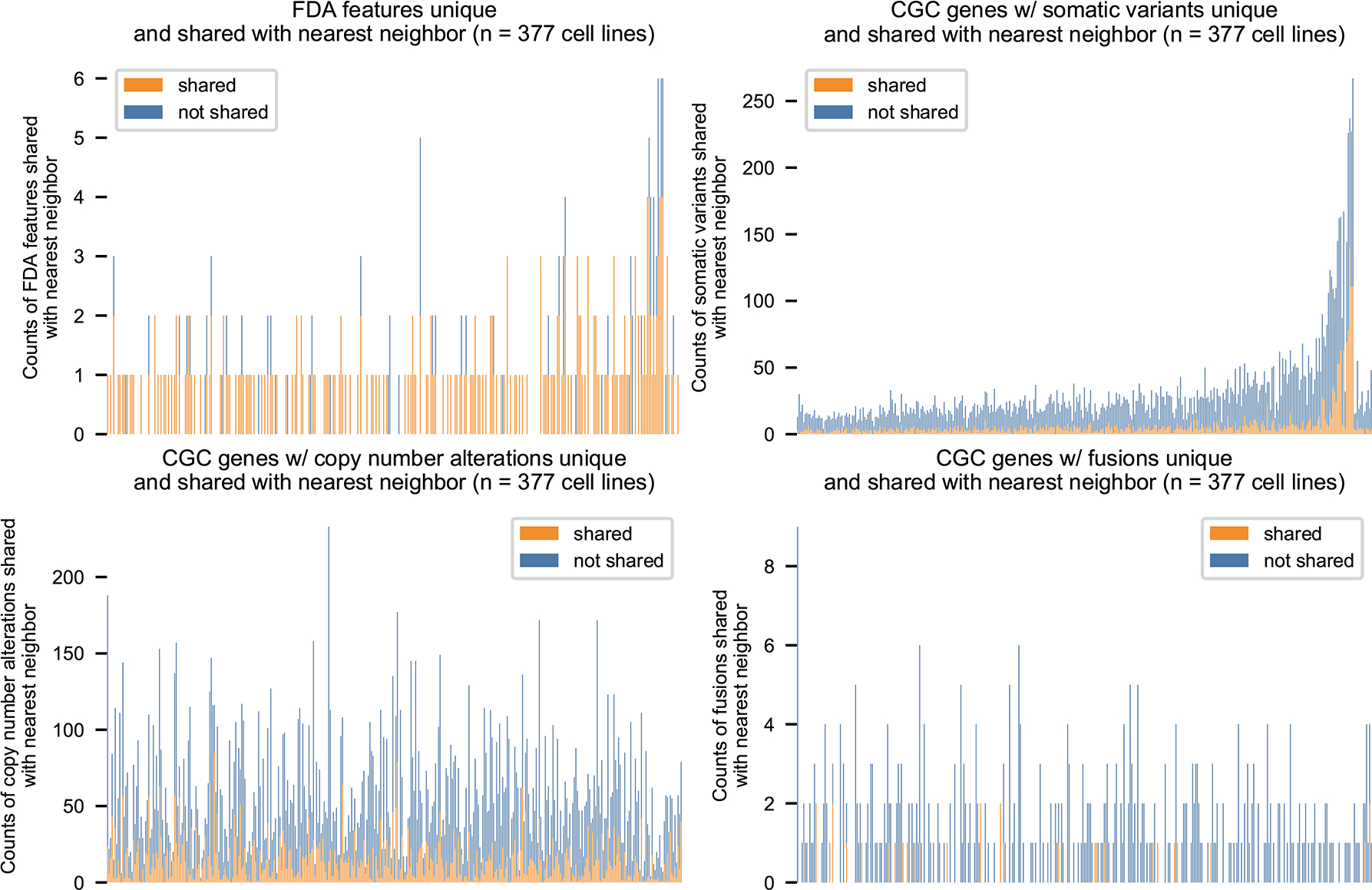
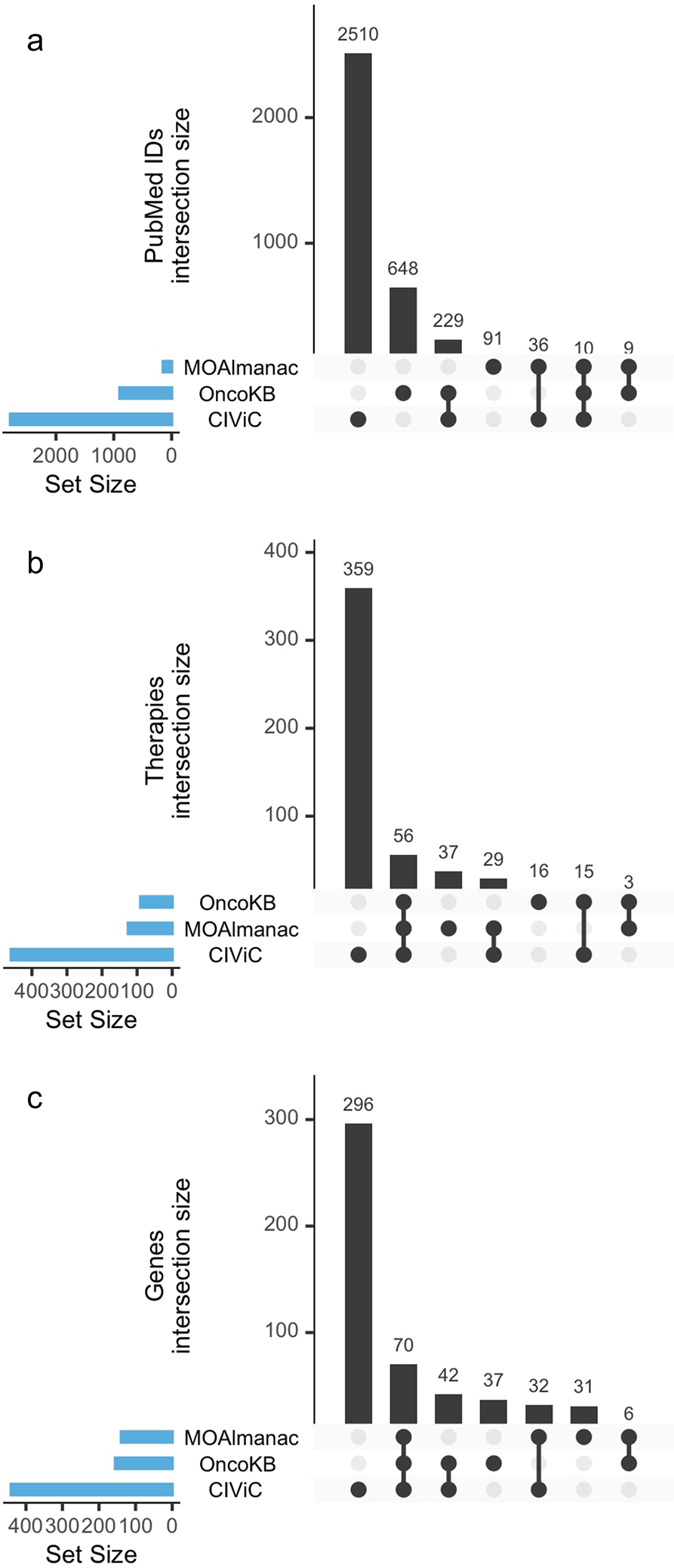
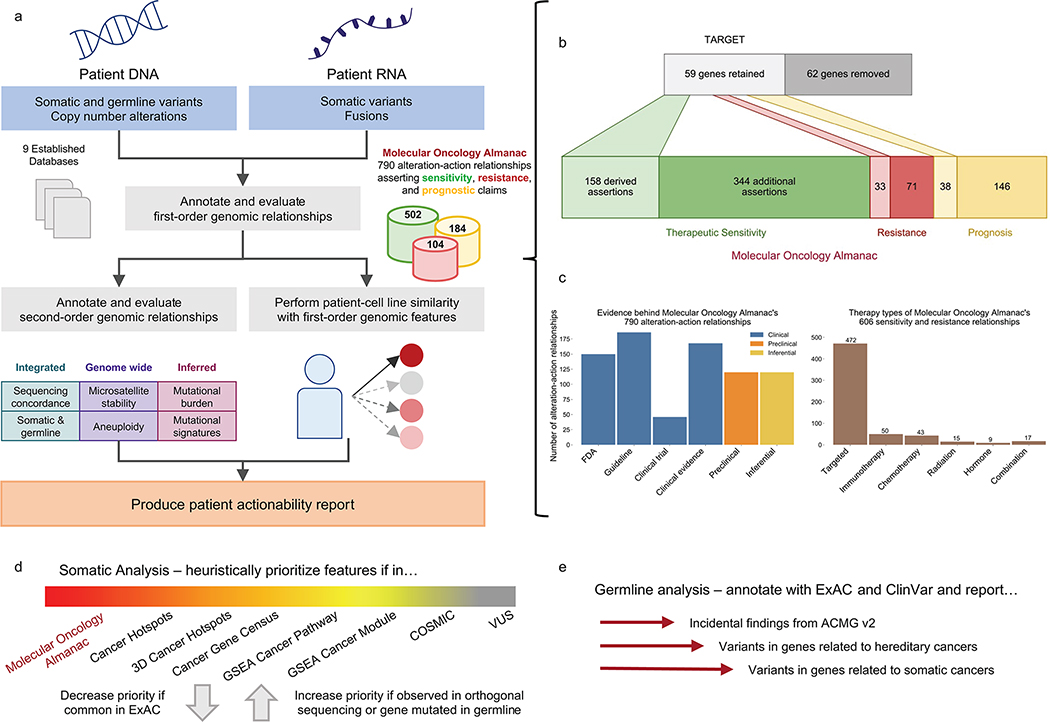
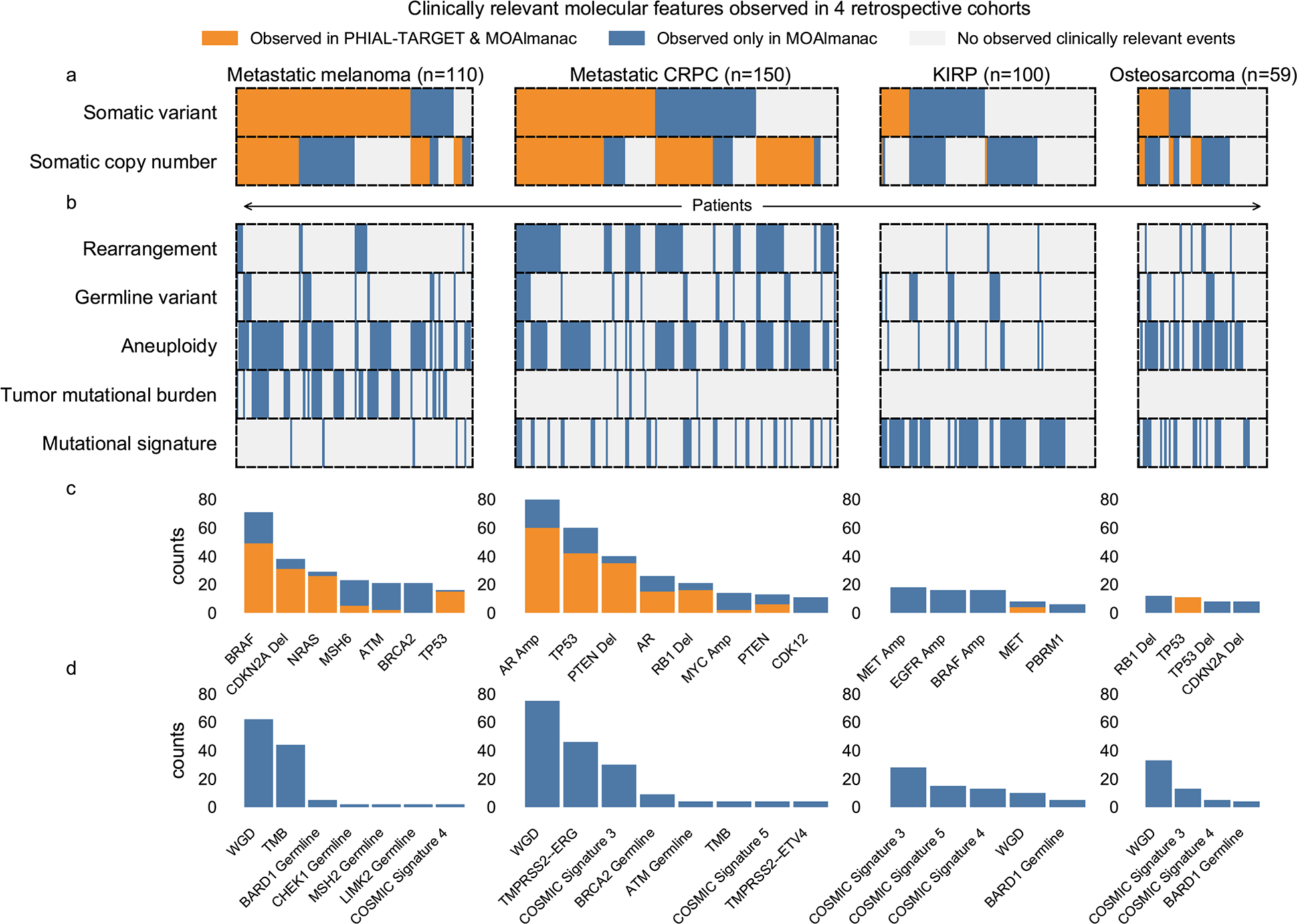
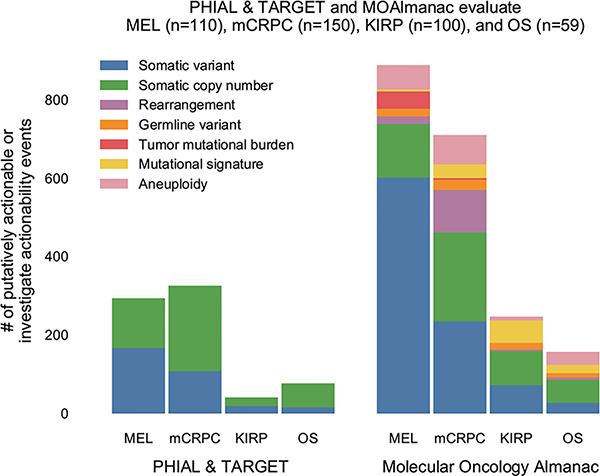
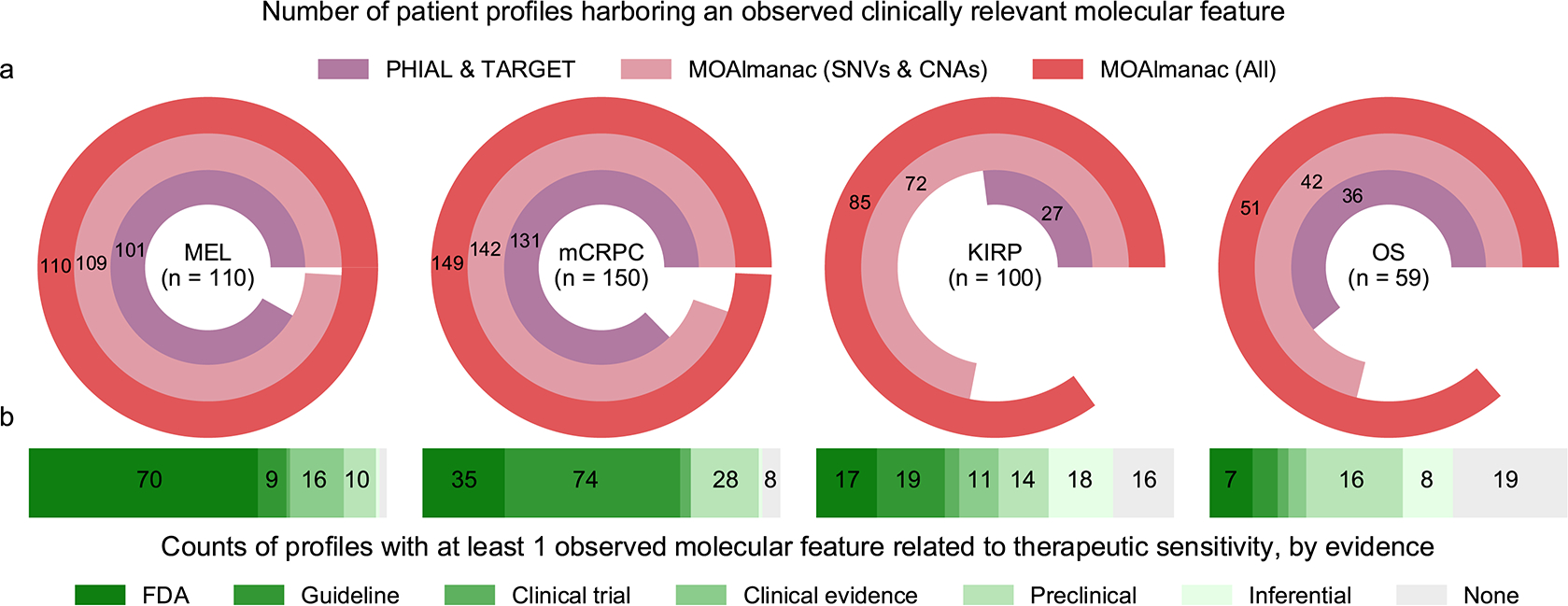
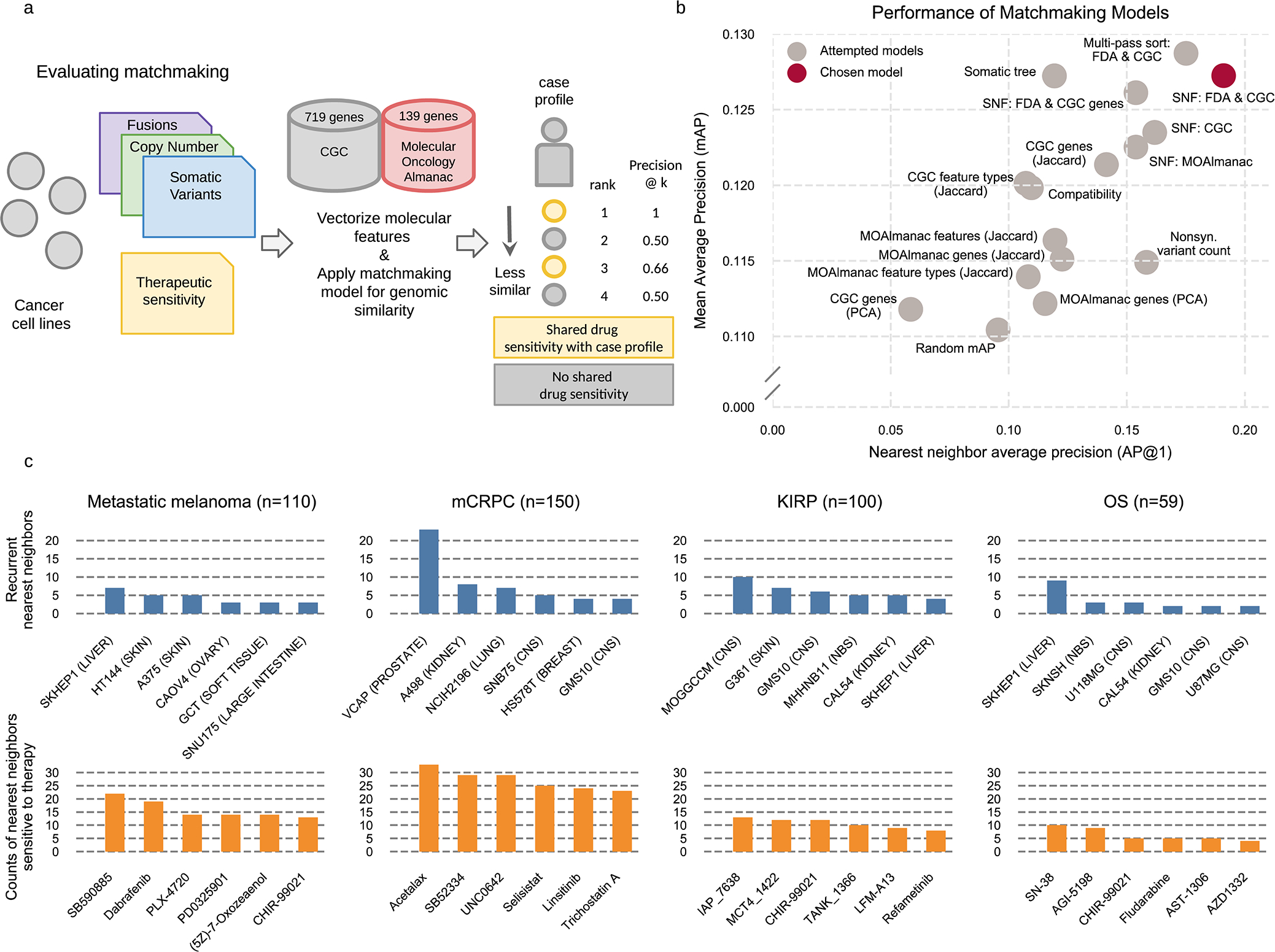
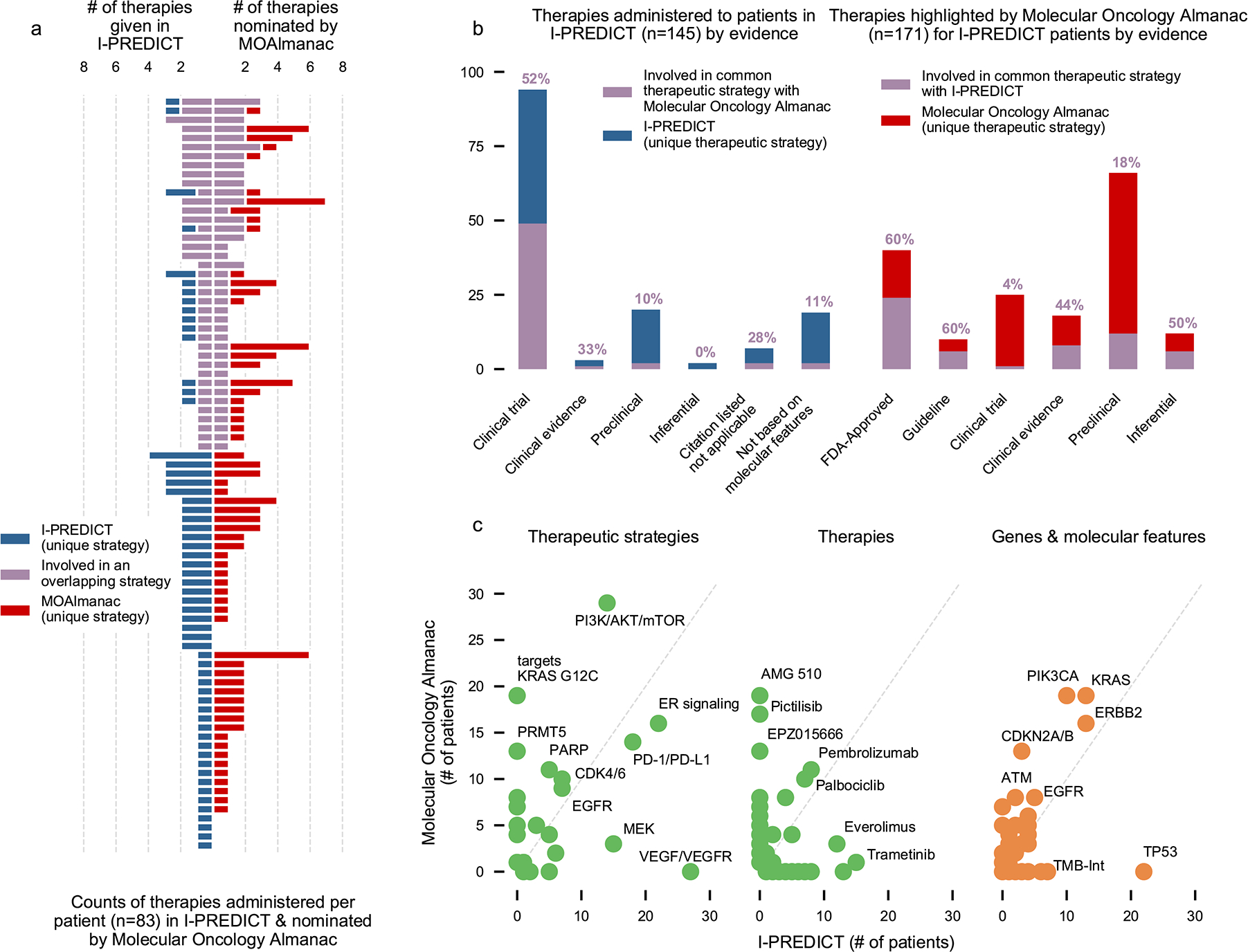
Tumor molecular profiling of single gene-variant ('first-order') genomic alterations informs potential therapeutic approaches. Interactions between such first-order events and global molecular features (for example, mutational signatures) are increasingly associated with clinical outcomes, but these 'second-order' alterations are not yet accounted for in clinical interpretation algorithms and knowledge bases. We introduce the Molecular Oncology Almanac (MOAlmanac), a paired clinical interpretation algorithm and knowledge base to enable integrative interpretation of multimodal genomic data for point-of-care decision making and translational-hypothesis generation. We benchmarked MOAlmanac to a first-order interpretation method across multiple retrospective cohorts and observed an increased number of clinical hypotheses from evaluation of molecular features and profile-to-cell line matchmaking. When applied to a prospective precision oncology trial cohort, MOAlmanac nominated a median of two therapies per patient and identified therapeutic strategies administered in 47% of patients. Overall, we present an open-source computational method for integrative clinical interpretation of individualized molecular profiles.
© 2021. The Author(s).
Conflict of interest statement
Competing interests statement
E.M.V.A. holds consulting roles with Tango Therapeutics, Genome Medical, Invitae, Enara Bio, Janssen, Manifold Bio, Monte Rosa. E.M.V.A. has received research support from Novartis, BMS. E.M.V.A. owns equity in Tango Therapeutics, Genome Medical, Syapse, Enara Bio, Manifold Bio, Microsoft, and Monte Rosa and has received travel reimbursement from Roche-Genentech. E.M.V.A., B.R., and N.D.M. have institutional patents filed on methods for clinical interpretation (international application number PCT/US2019/027338). N.I.V has served on the advisory board to Sanofi. The remaining authors declare no competing interests.
Figures
Comment in
-
A quick guide for clinical oncology.Nat Cancer. 2021 Oct;2(10):998-999. doi: 10.1038/s43018-021-00273-x. Nat Cancer. 2021. PMID: 35121881 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
